Introduction
Malaria in pregnancy (MiP) is a critical public health concern in sub-Saharan Africa, where it has been linked to a high prevalence of low birth weight, a major contributor to infant mortality.1–3 The highest prevalence of malaria exposure during pregnancy in 2022 was observed in Central and West Africa (40.1% and 39.3%, respectively),4 where many neonates were born with low birth weight, particularly in cases where pregnant women (PW) did not receive intermittent preventive treatment during pregnancy (IPTp).2 In 2023, an estimated 263 million malaria cases were reported globally across 83 endemic countries, primarily in the African region, which accounted for 94% of all cases.2 Malaria infection poses a substantial risk to PW, leading to adverse outcomes for both the mother and the fetus.5
Cameroon is 1 of 11 high-burden, high-impact countries where malaria accounts for 50% of hospitalisations and 19% of health facility deaths.6 7 While the proportional morbidity of malaria in the country decreased from 15.53% in 2018 to 10.9% in 2022,7 and maternal deaths dropped from 13.1 to 9.0 per 100 000 people in the same period,7 the coverage of three doses of IPTp using sulphadoxine-pyrimethamine (IPTp-SP) remains low.8 Evidence from Douala revealed persistent vulnerability, with higher malaria prevalence in pregnancy associated with younger maternal age (below 21 years) and not sleeping under mosquito bed nets.9 Consequently, the government of Cameroon continues to prioritise the fight against malaria as a public health emergency, as outlined in the country’s 2016–2027 Health Sector Strategy.6
Strategies for MiP control in Cameroon include IPTp-SP, insecticide-treated bed nets (ITNs) and case management in accordance with national policies.10–13 The 2022 Cameroon Malaria Indicator Survey highlighted that 65% of women had at least four antenatal care (ANC) visits, with a higher percentage in urban areas (75%) than in rural areas (56%)10; 63% of PW (14–49 years) slept under ITNs, with use being slightly higher among those in rural areas (65%) than in urban areas (60%).10 The 82.5% of women with a live birth who received one or more doses of SP/Fansidar for malaria prevention (79.0% in rural area vs 86.6% urban area) dropped to 45.8% for at least three doses (44.9% in rural areas against 46.9% in urban areas).10
In 2023, the percentage of PW attending first ANC who received ITNs was 87.4%; and IPTp distribution dropped from 80.5% for the first dose (IPTp1) to 51.3% for the third dose (IPTp3).7 Despite government efforts through specific interventions like ITNs, IPTp, malaria screening and treatment of detected cases, progress in reducing incidence and morbidity of malaria among PW has remained inconsistent. For example, from 2018 to 2022, there was a decrease from 2021 (incidence: 90.3%; proportional morbidity: 25.7%) to 2022 (incidence: 87.4%; proportional morbidity: 21.3%).7 While malaria remains a major cause of maternal mortality, the recent data from the National Strategic Plan 2024–2028 shows a drop in proportional mortality from 12.15% to 3.6% between 2019 and 2022 among PW.7 However, these figures must be interpreted in the context of significant implementation challenges, many of which were spillover effects of the COVID-19 pandemic. These include, for example, supply chain disruptions, delayed procurement of essential commodities and reduced attendance at health facilities, structural barriers such as poor and late ANC attendance, out-of-pocket costs and persistent service gaps, especially in rural areas, may constrain further, the effectiveness of malaria prevention strategies for PW.7 These challenges also highlight the urgent need for enhanced data collection, such as through digital systems, for timely monitoring and better planning of interventions.
Despite updated policy promoting monthly dosing of IPTp,14 many countries have not updated their ANC registers and/or electronic data platforms (eg, the District Health Information System 2, or DHIS2) to capture routine Health Management Information System (HMIS) data.1 Surveys like Demographic and Health Survey and Malaria Indicator Survey also provide data, but are more difficult and expensive to collect and are not used to drive ongoing programme management decisions.1 This is because these surveys are periodic and are not designed to provide real-time, timely data needed for daily operational management.
As Cameroon advances a digital health and universal health coverage agenda, its 2026–2030 National Digital Health Strategic framework aims to ensure that data are collected in electronic format and stored for routine follow-up.15 The framework aims to generate actionable and reliable data to improve quality of care and reduce morbidity and mortality by improving health outcomes through informed decision-making at all levels.15
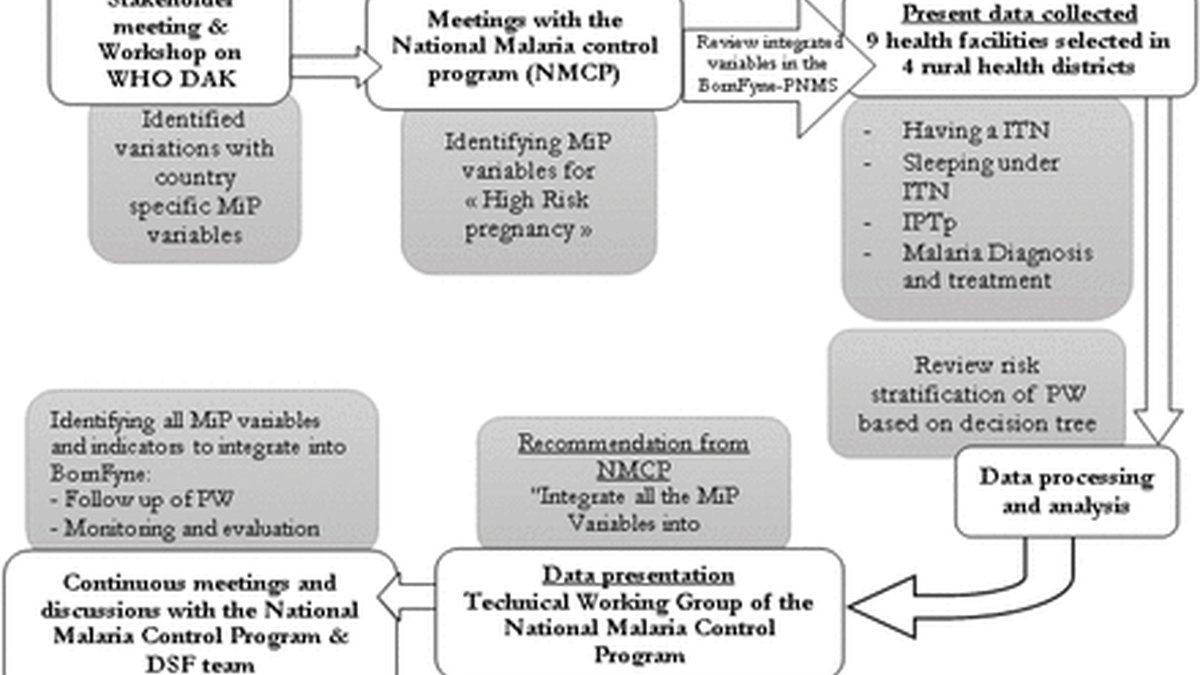
Generating timely, reliable, accurate and actionable data to inform decision-making and support the monitoring and evaluation of malaria programmes—particularly for MiP—remains a persistent challenge in Cameroon. Recognising the potential of digital platforms to address data gaps and enhance the generation of actionable data, the BornFyne digital health platform was identified by stakeholders to integrate MiP-specific variables into routine ANC.16–18 This platform was pilot-tested and presented to key stakeholders in 2023, to assess needs and identify strategies to strengthen the collection and use of reliable MiP data.16–18 This paper outlines the methodology used by the BornFyne team to engage stakeholders in identifying key MiP indicators for integration into an updated version of the BornFyne-PreNatal Management System (PNMS). It emphasises the critical role of stakeholder engagement for improved patient centric care and shares valuable lessons learnt throughout the participatory co-development process. Importantly, we detail the successful and sustained involvement of the Cameroon Ministry of Public Health (MoPH)—from initial planning through implementation, demonstrating how their leadership served as a driving force in identifying the MiP variables for integration. Furthermore, we illustrate how insights from this engagement informed the alignment of MiP data elements with the WHO’s ANC recommendations, as outlined in the WHO ANC Digital Adaptation Kit (DAK).19–22