I’ve taken agency in the treatment of my bone cancer (osteosarcoma in the T5 vertebrae of the upper spine). After I’ve ran out of standard of care treatment options and there were no trials available for me I’ve started doing: maximum diagnostics, created new treatments, started doing treatments in parallel, and scaling this for others.
Elliot Hershberg wrote a great and extensive article about my cancer journey.
My cancer journey deck is embedded below, there also is a recording of an OpenAI Forum presentation. The companies we are building to scale this approach for others can be found at evenone.ventures. Please scroll further on this page for my data and other information.
I think the medical industry can be more patient first, see this great article by Ruxandra https://www.writingruxandrabio.com/p/the-bureaucracy-blocking-the-chance
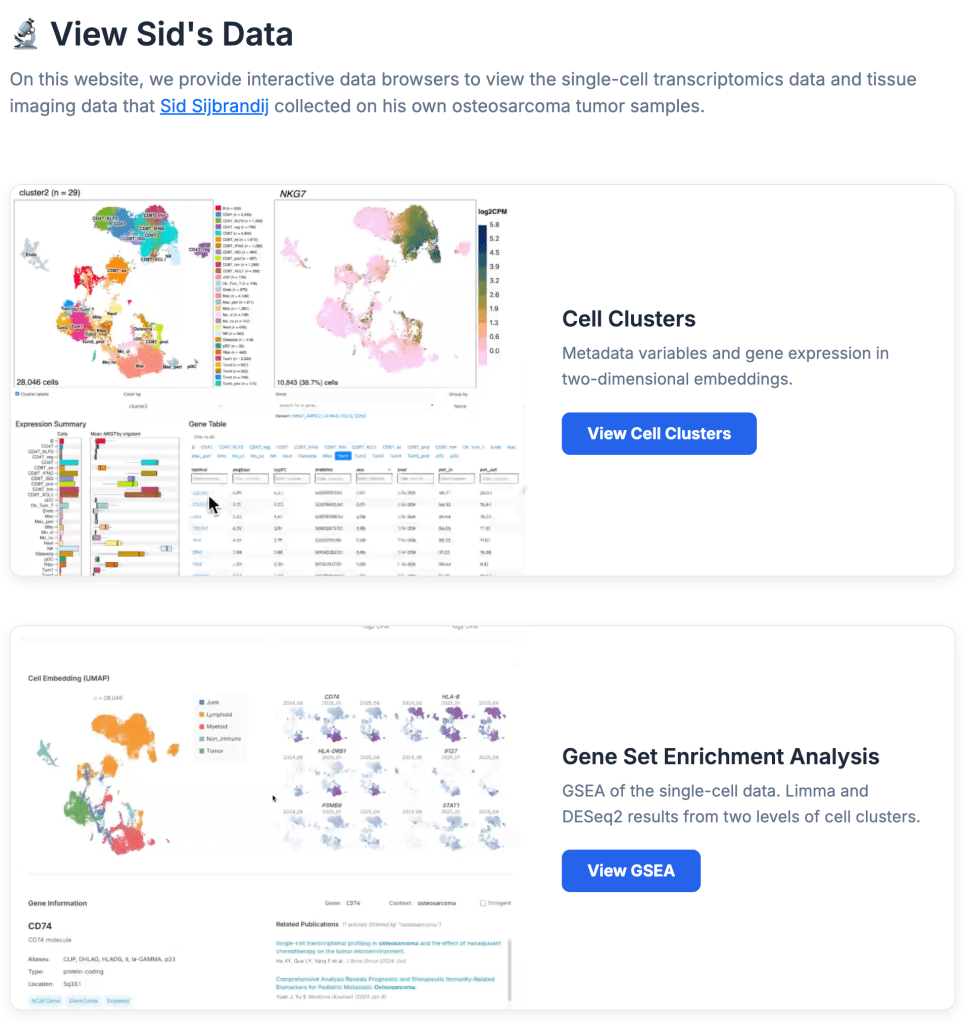
For my data please see https://osteosarc.com/ that includes my treatment timeline and a data overview doc with 25TB of publicly readable Google Cloud buckets.
Please subscribe to my mailing list
Contact me at cancer@sytse.com
Facts Only
A patient has osteosarcoma in the T5 vertebrae of the upper spine.
Standard treatment options were exhausted, and no clinical trials were available.
The patient conducted maximum diagnostics and created new treatments.
Treatments were implemented in parallel.
The patient is scaling this approach for others through evenone.ventures.
A cancer journey deck and OpenAI Forum presentation are publicly available.
Medical data, including a 25TB dataset, is accessible via osteosarc.com.
The patient references an article by Elliot Hershberg about their journey.
The patient critiques the medical industry’s bureaucratic barriers, citing an article by Ruxandra.
Contact information is provided: cancer@sytse.com.
A mailing list is available for updates.
Executive Summary
A patient with osteosarcoma in the T5 vertebrae of the upper spine has taken an active role in managing their treatment after exhausting standard options and finding no available clinical trials. They pursued extensive diagnostics, developed new treatments, and implemented parallel therapies while scaling this approach for others through ventures like evenone.ventures. The patient has documented their journey, including a 25TB dataset of medical records and treatment timelines, publicly accessible via osteosarc.com. They advocate for a more patient-centered medical industry, referencing critiques of bureaucratic barriers in cancer care. The patient also shares resources, including an article by Elliot Hershberg and a presentation from an OpenAI Forum, and encourages engagement through a mailing list and direct contact.
The narrative highlights a gap in traditional cancer care for patients who exhaust conventional treatments, emphasizing self-advocacy and data transparency. While the approach is innovative, it also raises questions about the scalability and safety of patient-driven treatment experimentation outside established medical frameworks. The patient’s efforts to democratize access to their methods and data reflect a broader push for patient empowerment in healthcare.
Full Take
This narrative presents a compelling case of patient agency in the face of systemic limitations in cancer care. The strongest version of this story is one of resilience and innovation—a patient taking control when traditional pathways fail, leveraging data transparency, and attempting to scale solutions for others. The emphasis on public data and collaborative ventures aligns with broader movements toward open science and patient-led healthcare.
However, the pattern scan reveals potential tensions. The critique of medical bureaucracy could be framed as a form of **ARC-0024 Ambiguity**, where systemic inefficiencies are highlighted without addressing the complexities of regulatory safeguards. The call for patient-first medicine, while laudable, risks oversimplifying the trade-offs between innovation and safety. There’s no overt manipulation, but the narrative leans into a **ARC-0043 Motte-and-Bailey** structure—advocating for patient empowerment (motte) while implicitly challenging established medical authority (bailey).
Root cause: The paradigm here is one of decentralized healthcare, where patients become active agents rather than passive recipients. Unstated assumptions include the belief that data transparency and parallel treatments can outpace institutional inertia. This echoes historical patterns of medical disillusionment, from HIV/AIDS activism to modern right-to-try movements.
Implications: For human agency, this is empowering—patients gain tools to fight beyond standard care. But costs include potential risks from unproven treatments and the burden of self-advocacy on those without resources. Second-order consequences may include pressure on institutions to adapt or resistance from regulators wary of untested methods.
Bridge questions: How might this model balance innovation with patient safety at scale? What structural changes in healthcare would make such self-advocacy less necessary? Could this approach widen disparities if only well-resourced patients can navigate it?
Counterstrike scan: A bad actor might exploit this narrative to undermine trust in medical institutions, framing bureaucracy as malicious rather than cautious. However, the content here focuses on solutions rather than blame, aligning more with constructive critique than coordinated attack. The emphasis on data sharing and collaboration suggests good faith.
Sentinel — Human
The text exhibits signs of human authorship, but also shows some indications of stylometric irregularities. The passage appears authentic due to the first-person narrative, personal experiences, and emotional engagement, as well as references to external articles and resources.