Discussion
This study, which conducted a multicountry analysis of 716 648 women aged 30–49 years across 44 LMICs, represents one of the largest and most geographically diverse investigations of the prevalence of premature or early menopause in resource-constrained settings. The standardised DHS methodology provides comparable, population-based estimates that help address knowledge gaps in women’s midlife health in LMICs.25
The overall pooled prevalence of premature or early menopause in this study was 7.1%, which is around 51 000 out of 716 648, a finding that substantially exceeds earlier global estimates predominantly derived from high-income country populations.26 27 Recent systematic reviews and meta-analyses have reported global premature ovarian insufficiency prevalence ranging from 3.5% to 3.7%, and our findings align more closely with the evidence suggesting higher burdens in LMICs specifically, where developing countries demonstrate premature ovarian insufficiency prevalence of 5.3% compared with 3.1% in developed nations.27 Moreover, secular trend analyses indicate an increasing prevalence of early and premature menopause in LMICs, particularly in sub-Saharan Africa and South/Southeast Asia.14 This divergent epidemiological trajectory has profound public health implications, as premature and early menopause are established risk factors for cardiovascular disease (1.5-fold increased risk of coronary heart disease, 1.3-fold increased risk of stroke), type 2 diabetes (1.3-fold increase), osteoporosis and fractures, neurological and psychiatric diseases, and premature mortality (1.2–1.3 fold increase).28 With populations in LMICs ageing rapidly and women expected to spend an increasing proportion of their lives in the postmenopausal state, the prevalence represents a substantial and growing burden on health systems already constrained by competing priorities and limited resources.29
At the country level, the observed sixfold variation in prevalence, ranging from 2.3% in Jordan to 12.0% in Ethiopia, underscores the substantial heterogeneity in menopause timing even within the LMIC context. The highest-prevalence countries (Ethiopia, Indonesia, Myanmar) represent diverse geographical regions and economic contexts, suggesting that local factors may outweigh broader regional or income-level determinants. Ethiopia’s higher prevalence may be partially explained by high rates of undernutrition, early marriage and childbearing practices, limited healthcare access in predominantly rural populations and elevated exposure to indoor air pollution from biomass fuel use.30 31 Conversely, the lowest-prevalence countries (Jordan, Gabon, Armenia) share characteristics including higher levels of urbanisation, better educational attainment and more developed healthcare infrastructure.17 32 Intriguingly, middle-income countries in the Middle East and North Africa region, where cultural factors strongly discourage early marriage and prioritise female education, demonstrated consistently lower prevalence rates.17
The consistent urban–rural disparity observed across all regions demands particular attention, as it reflects fundamental inequalities in healthcare access, nutritional status, educational opportunities and occupational exposures. Rural women consistently demonstrated a higher prevalence of premature or early menopause, and the final model confirmed they had higher odds of the condition compared with urban women. This pattern has been documented in individual country studies from India, Bangladesh and several systematic reviews from LMICs, and appears to operate through multiple pathways.16 31 33 34 Rural women in LMICs experience substantially higher rates of child marriage and early childbearing, both identified as independent associated factors for early menopause in our analysis.35 36 They face greater exposure to manual labour and occupational hazards, including agricultural chemicals, have limited access to primary healthcare services and preventive interventions, and experience higher rates of undernutrition and micronutrient deficiencies.35 37–39 Additionally, rural populations demonstrate lower health literacy regarding menopause and reproductive health, contributing to delays in seeking care and potentially exacerbating the health consequences of hormonal transitions.33 40 41 The persistence of this urban–rural gradient across diverse countries and regions suggests that addressing geographical inequalities in health system strengthening, education and social determinants must be central to any strategy aimed at improving women’s midlife health in LMICs.
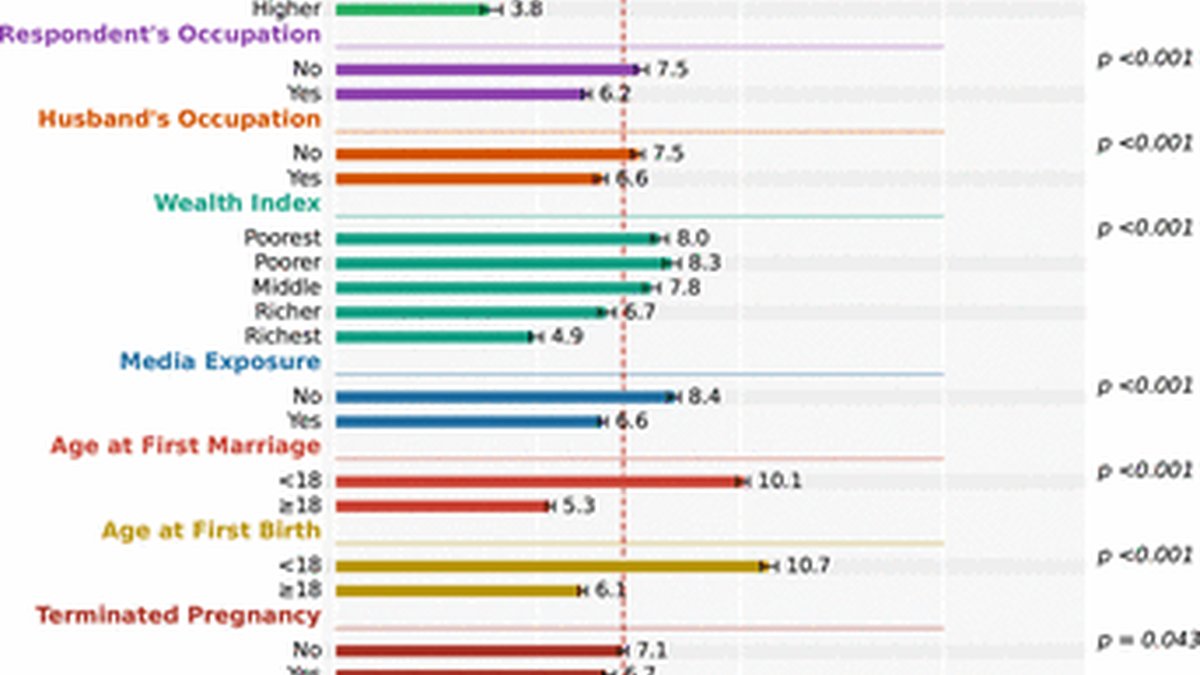
The study identified an inverse association between educational attainment and premature or early menopause: women with primary, secondary and higher education had progressively lower odds compared with those with no formal schooling, consistent with educational gradients in age at natural menopause reported in other settings.9 17 A systematic review across 24 countries reported that women with high versus low education experienced menopause approximately 7 months later on average, while a comprehensive Indian study revealed a sevenfold difference in premature menopause prevalence between educational extremes.17 42 Educational attainment may be protective through several pathways, including better health literacy and engagement with healthcare, which can reduce unnecessary gynaecological surgery, and more favourable socio-economic conditions that improve nutrition, reduce chronic stress and lower lifetime exposure to reproductive health risks.17 32 Together, this suggests that educational interventions targeting girls represent upstream preventive approaches, addressing premature menopause decades before reproductive senescence becomes apparent.
The study reveals that employed women experience substantially lower odds of menopause, a finding reflecting both material economic benefits and important psychosocial mechanisms beyond simple income provision. While employment provides obvious advantages, improved healthcare access, enhanced nutrition and reduced financial stress, recent research on menopause in occupational settings highlights that meaningful employment, particularly roles offering decision-making autonomy and skill development, preserves women’s self-efficacy, social integration and sense of purpose during reproductive transition.43–45 However, reverse causation demands careful consideration, as women experiencing premature menopause and its associated morbidity (vasomotor symptoms, mood disturbances, chronic disease) face a higher risk of workforce exit, suggesting that the observed protection may partially reflect healthier women’s greater likelihood of employment retention. Additionally, employment quality matters critically; occupational exposures, including heavy manual labour, agricultural chemicals, shift work and chronic stress, can accelerate rather than delay reproductive ageing.19 43 This finding suggests that the observed association between employment and lower odds of menopause may reflect, in part, material and psychosocial advantages associated with employment; however, the present study did not assess employment quality or workplace exposures. Therefore, the role of occupational characteristics in shaping reproductive ageing should be examined in future research.
The study found that, although the richer and richest wealth groups showed a lower crude prevalence of premature or early menopause in the bivariate analysis, this pattern reversed after adjustment for other covariates in the multivariable model. This shift suggests that the observed protective association between greater wealth and the unadjusted comparisons was at least in part due to the influence of other variables that are strongly associated with socio-economic position.17 The analysis also indicates that women in middle wealth categories carried the highest likelihood, pointing to a non-linear association between household wealth and premature or early menopause that is consistent with evidence from LMICs on wealth–body mass index (BMI) correlations and nutritional transition.46 47 In these settings, women in intermediate wealth groups are more likely to experience rapid increases in BMI and metabolic risk, as well as greater access to surgical care without guaranteed access to high-quality conservative gynaecological management, which may increase the likelihood of iatrogenic menopause.47 48 Together, these findings underscore that household wealth does not operate as a simple linear protective factor and that careful adjustment for correlated social and health factors is essential when interpreting socio-economic gradients in reproductive ageing. These patterns also highlight the broader challenges of measuring socio-economic position in LMICs, where both income and asset-based indicators provide only partial views of women’s social and economic circumstances.
The study identified that women initiating marriage and childbearing before age 18 face substantially higher odds of premature or early menopause, reflecting both direct biological consequences of adolescent reproduction and powerful socio-economic confounding. Early pregnancy before full pelvic maturity creates nutritional competition between growing adolescent bodies and developing fetuses, precipitating maternal depletion, elevated obstetric complications and a higher likelihood of surgical interventions that compromise ovarian function.49 Adolescent sexual debut amplifies cumulative exposure to sexually transmitted infections, causing pelvic inflammatory disease and chronic reproductive tract morbidity that progressively impairs ovarian reserve.50 Beyond biology, early marriage and childbearing represent markers of profound socio-economic disadvantage: these practices cluster with low education, poverty, rural residence and limited healthcare access, creating what researchers term an intersectionality of vulnerabilities.49 50 The social determinism underlying early reproduction in resource-constrained settings, including patriarchal constraints on girls’ autonomy, limited secondary education access and economic pressures, thus establishes life-long trajectories of reproductive and metabolic disadvantage.49 51 A previous study found that early marriage often leads to earlier childbearing, which is linked to menopausal timing, and these increase the risk of premature or early menopause due to shorter reproductive lifespan or increased physiological stress.16
The study also found that women with three or more children had a lower odds of premature or early menopause than those with one or two children, a pattern that aligns with evidence from multiple populations. This protective parity effect, consistently documented across diverse populations, reflects the fundamental biology of ovulation suppression: each pregnancy prevents approximately 9–12 months of ovulation, while breastfeeding extends the anovulatory period 6–24 months, depending on exclusivity and duration.52 Since menopause results from ovarian follicle pool depletion through progressive recruitment and atresia, reproductive events that suppress ovulation preserve ovarian reserve by slowing follicular loss.53 54 Nulliparous women, lacking this protective mechanism, experience uninterrupted monthly follicular recruitment and depletion, reaching the menopause threshold earlier.55 This ovulation-suppression mechanism implies that reproductive events can preserve ovarian reserve by reducing the number of cycles in which follicles are recruited and undergo atresia.52 56 Observational studies consistently report that parous women, especially those with multiple births, tend to experience menopause later than nulliparous women, who lack these ovulation-free intervals and therefore accumulate more cycles of follicular loss over time.52 57.
Policy implications and recommendations
The geographical variations of early or premature menopause highlight the critical need for context-specific interventions and policies that address the unique determinants operating in different settings. The high prevalence in certain regions and countries, combined with the well-established health consequences of early menopause, demands urgent integration of menopause into existing reproductive health and NCD prevention frameworks in LMICs. Notably, countries such as Ethiopia, Indonesia and Myanmar, as well as the South Asia and East Asia and Pacific regions, require immediate prioritisation given their disproportionate burden. Current health policies in most LMICs remain silent on menopause, with limited provider training, absent screening protocols and inadequate access to evidence-based treatments, including menopausal hormone therapy. Addressing this gap requires multilevel interventions spanning health system strengthening (provider education, clinical guidelines, essential medicines lists), community-level interventions (health literacy campaigns, culturally appropriate educational materials) and upstream social determinants, including girls’ education, delayed marriage and childbearing, improved nutrition and economic empowerment of women.
Given the marked educational gradient observed, policies that prioritise universal completion of secondary education for girls represent a critical upstream intervention, as higher education not only delays marriage and first birth but also enhances health literacy and reduces reliance on hysterectomy for treatable gynaecological conditions. The higher odds associated with early marriage and childbearing before age 18 underscore the urgent need to enforce and operationalise laws against child marriage, coupled with social protection programmes such as conditional cash transfers and community mobilisation that enable families to delay marriage and support girls’ educational attainment. Furthermore, the persistent urban–rural disparity, which was evident across all regions but particularly pronounced in South Asia and East Asia and Pacific, calls for targeted investment in rural primary healthcare infrastructure, including training community health workers to recognise early menopause symptoms. Additionally, workplace policies that recognise menopause as a legitimate occupational health concern, including flexible work arrangements, reasonable accommodations for severe symptoms and protections against employment discrimination, are essential to support employed women and prevent premature workforce exit, particularly in countries like Indonesia, Bangladesh and South Africa, where large female workforces are emerging in both formal and informal sectors.
Future research must prioritise establishing nationally representative menopause surveillance systems within existing DHSs, particularly in high-burden regions such as South Asia, East Asia and Pacific and sub-Saharan Africa, conducting prospective cohort studies to elucidate causal pathways linking early-life disadvantage with reproductive ageing, investigating region-specific determinants through mixed-methods approaches that incorporate women’s and providers’ perspectives, and evaluating implementation strategies for evidence-based menopause care adapted to resource-constrained settings, with particular attention to cost-effectiveness and equity impacts.
Strengths and limitations
This study has several notable strengths. First, it represents the largest and most geographically diverse multicountry analysis examining the pooled prevalence and determinants of premature or early menopause across 44 LMICs using the most recent DHS data. Second, the standardised DHS methodology ensures cross-country comparability through uniform sampling procedures, questionnaire design and data collection protocols, enhancing the validity of pooled estimates and cross-national comparisons. Third, the study systematically examined urban–rural disparities across all countries and documented substantial variations by geographical region and income level, providing granular insights into the social and spatial patterning of early menopause that can inform targeted interventions. Finally, the findings can inform national and regional policymakers to address shared challenges while designing context-specific interventions tailored to local determinants and health system capacities.
Nonetheless, several important limitations need to be acknowledged. First, the cross-sectional design precludes establishing temporal sequence and causal inference between exposures and premature or early menopause; reverse causation and unmeasured confounding may partially explain observed associations. Second, reliance on self-reported data introduces potential recall bias, especially regarding age at last menstrual period and reproductive history, as well as social desirability bias in reporting sensitive behaviours such as marriage and childbearing age. Third, the operational definition of premature or early menopause, while aligned with DHS guidelines and prior research, cannot distinguish natural from surgical menopause caused by hysterectomy or oophorectomy in all cases, potentially overestimating prevalence in settings with high rates of gynaecological surgery. Fourth, menopause status was operationalised using the DHS criterion of at least 6 months since the last menstrual period, which differs from the WHO-recommended 12-month definition and may misclassify some women, particularly those with irregular cycles or using hormonal methods. Although a sensitivity analysis applying a 12-month amenorrhea threshold yielded very similar pooled prevalence estimates and patterns of association, some residual misclassification is likely and could bias estimates towards the null. In addition, our outcome definition may misclassify some women using hormonal contraceptive methods that induce amenorrhoea, particularly long-acting injectables, as menopausal under the 6-month criterion, because it is not always possible to distinguish contraceptive-induced amenorrhoea from natural menopause in cross-sectional DHS data. Descriptive analyses of premature or early menopause by current contraceptive method (online supplemental table 7) showed a higher proportion classified as menopausal among injectable users, suggesting that prevalence may be modestly overestimated in settings where these methods are common. Fifth, survival bias may underestimate true prevalence if women experiencing premature menopause and its associated cardiovascular and metabolic sequelae have reduced survival to survey ages, particularly in low-income countries with limited healthcare access. Sixth, the study could not include several important variables associated with menopause timing, including smoking, alcohol consumption, physical activity, dietary quality, chronic disease burden, hormonal contraceptive use, breastfeeding duration and environmental exposures, because these are not consistently measured across DHS surveys. Seventh, although the DHS uses a standardised survey platform, important heterogeneity still exists across countries in terms of social context, survey year, the age distribution of women 30–49 years, health-system access and the prevalence of unmeasured determinants of menopause timing. Eighth, DHS data availability excluded countries without recent surveys or complete reproductive health modules, potentially limiting generalisability to all LMICs, particularly in Latin America, Central Asia and the Middle East. Finally, we used the household wealth index as our primary indicator of socio-economic status because individual income is not collected and is often unreliable in DHS and similar surveys in LMICs. While wealth indices capture long-term material living standards, they may not fully reflect women’s own economic autonomy or lifetime socio-economic trajectories, and like income, they have known limitations as proxies for socio-economic position in health research. Consequently, our findings on socio-economic gradients in premature or early menopause should be interpreted as reflecting broad relative position rather than precise, individual-level economic resources. Despite these limitations, the study provides the most comprehensive evidence to date on premature or early menopause across LMICs and establishes a foundation for future longitudinal, biomarker-enhanced research in this underinvestigated area of women’s health.