Abstract
Incretins have improved the management of obesity and its related complications, but maintaining these health benefits requires ongoing administration, which can be challenging. Orforglipron, a once-daily oral nonpeptide glucagon-like peptide-1 (GLP-1) receptor agonist, has demonstrated weight loss efficacy, improvements in cardiometabolic risk factors, and safety generally similar to injectable GLP-1 receptor agonists. Here this double-blind, placebo-controlled trial randomized participants previously treated with tirzepatide (cohort 1: N = 205) or semaglutide (cohort 2: N = 171) during the SURMOUNT-5 study to orforglipron once daily or placebo. Cohort 1 participants who achieved body weight plateau maintained a model-based estimate (MBE) of 74.7% (s.e.m. 4.05) of body weight reduction with orforglipron compared with an MBE of 49.2% (s.e.m. 3.92) with placebo, resulting in an estimated treatment difference of MBE 25.5% (95% confidence interval 14.5 to 36.5); P < 0.001; treatment-regimen estimand) at week 52. Cohort 2 participants who achieved body weight plateau maintained an MBE of 79.3% (s.e.m. 4.42) of body weight reduction with orforglipron compared with an MBE of 37.6% (s.e.m. 7.46) with placebo, resulting in an estimated treatment difference of MBE 41.7 (95% confidence interval 24.4 to 59.0); P < 0.001; treatment-regimen estimand) at week 52. All key secondary endpoints were met. The most common adverse events were gastrointestinal effects, which were mostly mild to moderate in severity. These data demonstrate orforglipron’s potential as a globally scalable option for minimizing weight changes after injectable therapy. Trial limitations include the absence of a comparator arm involving continued use of injectable obesity-management medications and the trial’s 1-year duration. ClinicalTrials.gov registration: NCT06584916.
Similar content being viewed by others
Main
Obesity is a chronic, relapsing and treatable multifactorial disease1. Although safe and effective therapies are now available, persistence with existing injectable obesity management medications (OMMs) remains a barrier to weight loss maintenance2. Weight regain after discontinuing weight loss interventions, regardless of modality of weight loss, has been demonstrated, underscoring the need for sustained therapy to minimize changes in body weight and retain improvements in cardiometabolic parameters after weight reduction with the ultimate goal of preserving the accompanying benefits to overall health3,4.
Weight regain can be associated with negative overall health consequences, such as reversal of cardiometabolic improvement, impaired physical function (for example, increased pain) and an increase in psychological burden. During the weight maintenance phase, weight regain can occur secondary to decreased energy expenditure and increased energy efficiency, which together result in a net decrease in caloric needs5,6,7,8. Because of the negative consequences of weight regain and weight cycling, utilizing options to minimize weight change after intentional weight loss is a vital component for successful long-term health outcomes. As more options for safe and effective OMMs become available, exploring their role in preserving weight loss and minimizing weight change will help patients to receive evidence-based care across all phases of obesity management.
Orforglipron is a once-daily, nonpeptide GLP-1 receptor agonist (RA) currently under investigation for the treatment of obesity and type 2 diabetes. The ATTAIN global phase 3 registration program demonstrated clinically significant and meaningful body weight reduction along with improvements in markers of cardiometabolic disease, such as waist circumference, blood pressure, lipids and high‑sensitivity C‑reactive protein, in people with obesity, with and without type 2 diabetes, with an efficacy and safety profile generally similar to injectable incretin-based OMMs3,9. As a nonpeptide oral therapy, orforglipron has the potential to eliminate some individual patient barriers to injectable therapy (for example, resistance to injection, increased challenges with traveling, cold chain distribution and so on), can be taken without food or water restrictions and, if approved, can be globally scalable to meet the need for treatments worldwide. Literature suggests that aligning with patients’ preferences of attributes in treatment modalities increases the likelihood of patients persisting on therapy10,11. Thus, by addressing barriers that can be alleviated by orforglipron, generating evidence of its ability to maintain body weight reduction, along with safety data when switching to oral therapy, can help advance the field of obesity medicine.
The aim of this study was to assess the efficacy and safety of orforglipron compared with placebo, in maintenance of body weight reduction after 72 weeks of tirzepatide (cohort 1) or semaglutide (cohort 2) treatment in participants with obesity or body mass index (BMI) ≥27 kg/m2 with obesity-related complications who had previously participated in the SURMOUNT-5 study12. This is the initial clinical trial investigating the switch from injectable incretin-based therapy to an oral OMM for the maintenance of body weight reduction, and as a result, the study evaluated various endpoints, acknowledging that the clinical relevance of these endpoints may not be appreciated until trial completion. This study addressed important clinical questions, including a dosing strategy to transition patients from injectable to oral therapy, tolerability during the transition, and whether switching to oral therapy helps preserve the weight reduction achieved after injectable therapy compared with discontinuing therapy.
Results
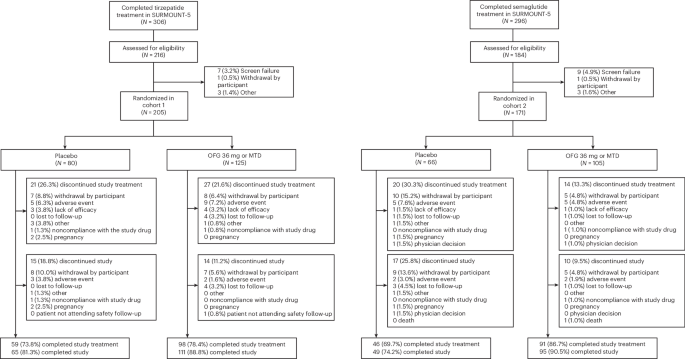
ATTAIN-MAINTAIN screened 400 and enrolled 376 participants between 13 September 2024 and 21 November 2025, in 29 sites in the USA. A total of 205 participants in cohort 1 were randomized to treatment (N = 125 orforglipron 36 mg or maximum tolerated dose (MTD), N = 80 placebo) and 171 participants in cohort 2 were randomized to treatment (N = 105 orforglipron 36 mg or MTD, N = 66 placebo) (Fig. 1). This work reports data on the investigational orforglipron capsule formulation of 1, 3, 6, 12, 24 and 36 mg; the doses have been shown as the equivalent to tablet doses of 0.8, 2.5, 5.5, 9, 14.5 and 17.2 mg, respectively, which are approved in the USA13. Overall, 157 (76.6%) participants in cohort 1 and 137 (80.1%) participants in cohort 2 completed study treatment, and 176 (85.9%) completed the study in cohort 1 and 144 (84.2%) in cohort 2. Reasons for early study treatment and study discontinuations are shown in Fig. 1. Table 1 presents the demographic and baseline characteristics of the participants. In cohort 1, the mean age of the participants was 48.5 years; most were female (62.9%) and white (73.8%) and had a mean body weight of 90.1 kg. In cohort 2, the mean age was 48.6 years; most participants were female (68.4%) and white (75.9%) and had a mean body weight of 94.4 kg.
Cohort 1: tirzepatide to orforglipron (MTD) versus placebo
For the primary endpoint with the modified treatment-regimen estimand, participants in cohort 1 who achieved body weight plateau (<5% body weight change from weeks 60 to 72 in the SURMOUNT-5 study) maintained 74.7% (s.e.m. 4.05) of body weight reduction with orforglipron compared with 49.2% (s.e.m. 3.92) with placebo, with an estimated treatment difference (ETD) relative to placebo of 25.5% (95% confidence interval (CI) 14.5 to 36.5); P < 0.001) at week 52. Key secondary endpoints in the modified treatment-regimen estimand, in cohort 1 participants who achieved a body weight plateau, 43.7% (s.e.m. 4.98) of participants treated with orforglipron maintained ≥80% of the body weight reduction achieved during SURMOUNT-5 compared with 16.4% (s.e.m. 4.60) with placebo, with a risk difference to placebo of 27.3 (95% CI 14.1 to 40.6); P < 0.001 (efficacy estimand data shown in Extended Data Fig. 1a). All participants in cohort 1 maintained 74.4% (s.e.m. 3.63) of body weight reduction with orforglipron and 49.7% (s.e.m. 3.53) with placebo, with an ETD relative to placebo of 24.7 percentage points (95% CI 14.9 to 34.5; P < 0.001) with orforglipron treatment. All participants in cohort 1 had a mean MBE percent change from SURMOUNT-5 baseline body weight of –16.5% (s.e.m. 0.90) with orforglipron and 12.6% (s.e.m. 0.91) with placebo with an ETD relative to placebo of –3.9 percentage points (95% CI –6.1 to –1.8; P < 0.001).
In additional sensitivity analyses based on the efficacy estimand, participants in cohort 1 randomized only to orforglipron in ATTAIN-MAINTAIN had a mean baseline body weight of 115.8 kg (s.e.m. 2.23) in SURMOUNT-5. At the start of the ATTAIN-MAINTAIN study, they had a baseline body weight of 90.9 kg (s.e.m. 2.12) with a reduction of 21.5% (s.e.m. 0.83). Participants in cohort 1 had a mean MBE body weight reduction of 16.8% (s.e.m. 0.76) (Fig. 2a) and absolute body weight reduction of 19.6 kg (s.e.m. 0.91) (Fig. 2b) from the beginning of SURMOUNT-5 to the end of ATTAIN-MAINTAIN. This represents a difference in percent weight changes of approximately 5% and an average difference in weight of approximately 5 kg from baseline. For these participants, the mean body weight (MBE) at week 52 was 95.9 kg (s.e.m. 0.91) with orforglipron (Fig. 2c). Participants in cohort 1 at 24 weeks, before rescue therapy eligibility per study protocol, had a mean MBE body weight reduction of −19.0% (s.e.m. 0.68) from the beginning of SURMOUNT-5, with a mean MBE body weight of 93.4 kg (s.e.m. 0.79). This preserved the previously achieved weight reduction with an average difference of approximately 3 kg. Among all participants in cohort 1 randomized only to orforglipron who achieved 15% or more body weight reduction in SURMOUNT-5, 63.7% (s.e.m. 5.03) maintained 15% or more body weight reduction after 52 weeks of treatment with orforglipron.
Participants in cohort 1 randomized only to orforglipron in ATTAIN-MAINTAIN had a mean baseline waist circumference of 120.8 cm (s.e.m. 1.48) in SURMOUNT-5. At the start of the ATTAIN-MAINTAIN study, they had a mean waist circumference of 100.3 cm (s.e.m. 1.50) with a decrease in mean waist circumference of 20.5 cm (s.e.m. 0.95) (Extended Data Fig. 2a,b). Based on the efficacy estimand, participants in cohort 1 had a mean decrease in waist circumference of 16.3 (s.e.m. 0.86) cm from the beginning of SURMOUNT-5, resulting in an MBE waist circumference of 103.4 cm (s.e.m. 0.86) with orforglipron. This preserved their previously achieved decrease in waist circumference with an average change from randomization of approximately 3 cm (Extended Data Fig. 2a).
In addition, other cardiometabolic risk factors demonstrated similar preservation of reductions at the end of ATTAIN-MAINTAIN. As an example, in cohort 1, participants subsequently randomized to orforglipron had a mean baseline HbA1c of 5.6% at the beginning of SURMOUNT-5. At the beginning of ATTAIN-MAINTAIN, after weight reduction with injectables, the HbA1c improved to a mean of 5.2%. At 52 weeks, the mean HbA1c remained at 5.2% and retained the improvements in this marker after switching to oral orforglipron. Similar trends were observed in insulin levels, fasting serum glucose (FSG), markers of lipids such as triglycerides and non-HDL, and systolic blood pressure (Extended Data Fig. 3a–e).
Cohort 2: semaglutide to orforglipron (MTD) versus placebo
For the primary endpoint with modified treatment-regimen estimand, participants in cohort 2 who achieved body weight plateau maintained 79.3% (s.e.m. 4.42) of body weight reduction with orforglipron compared with 37.6% (s.e.m. 7.46) with placebo, with an ETD relative to placebo of 41.7 (95% CI 24.4 to 59.0); P < 0.001) at week 52. Among key secondary endpoints in cohort 2, participants who achieved a body weight plateau, 55.0% (s.e.m. 5.08) of those treated with orforglipron maintained ≥80% of the body weight reduction achieved during SURMOUNT-5, compared with 6.9% (s.e.m. 3.77) with placebo, corresponding to a risk difference of 48.1 (95% CI 35.6 to 60.5; P < 0.001) (efficacy estimand data shown in Extended Data Fig. 1b). All participants in cohort 2 maintained 85.9% (s.e.m. 4.60) of body weight reduction with orforglipron and 40.2% (s.e.m. 7.87) with placebo, with an ETD relative to placebo of 45.6 percentage points (95% CI 28.3 to 63.0; P < 0.001) with orforglipron treatment. All participants in cohort 2 had a mean MBE percent change from SURMOUNT-5 baseline body weight of –14.9% (s.e.m. 0.94) with orforglipron and –7.9% (SE 0.81) with placebo, with an ETD relative to placebo of –7.0 percentage points (95% CI –9.1 to –5.0; P < 0.001).
In additional sensitivity analyses of the efficacy estimand, participants in cohort 2 randomized only to orforglipron in ATTAIN-MAINTAIN had a mean baseline body weight of 113.5 kg (s.e.m. 2.64) in SURMOUNT-5. At the start of the ATTAIN-MAINTAIN study, they had a baseline body weight of 95.0 kg (s.e.m. 2.51) with a reduction of 16.5% (s.e.m. 0.81). Participants in cohort 2 had a mean MBE body weight reduction of 15.1% (s.e.m. 0.67) (Fig. 3a) and absolute body weight reduction of 17.1 kg (Fig. 3b) from the beginning of SURMOUNT-5 to the end of ATTAIN-MAINTAIN. This represents a difference in percent weight change of approximately 1% and an average difference in weight of approximately 1 kg from baseline. For these participants, the mean body weight (MBE) at week 52 was 95.9 kg (s.e.m. 0.76) with orforglipron (Fig. 3c). Participants in cohort 2 at 24 weeks, before rescue therapy eligibility per study protocol, had a mean MBE body weight reduction of 16.3% (s.e.m. 0.56) from the beginning of SURMOUNT-5, with a mean MBE body weight of 94.5 kg (s.e.m. 0.68). This preserved all of the previously achieved weight reduction. Among all participants in cohort 2 randomized only to orforglipron who achieved 15% or more body weight reduction in SURMOUNT-5, 69.5% (s.e.m. 5.79) maintained 15% or more body weight reduction after 52 weeks of treatment with orforglipron.
Participants in cohort 2 randomized only to orforglipron in ATTAIN-MAINTAIN had a mean baseline waist circumference of 119.1 cm (s.e.m. 1.77) in SURMOUNT-5. At the start of the ATTAIN-MAINTAIN study, they had a waist circumference of 103.4 (s.e.m. 1.83) cm with a decrease in mean waist circumference of 15.6 (s.e.m. 1.09) cm (Extended Data Fig. 2c,d). Based on the efficacy estimand, participants in cohort 2 had a mean decrease in waist circumference of 14.2 (s.e.m. 0.90) cm from the beginning of SURMOUNT-5, resulting in an MBE waist circumference of 104.5 (s.e.m. 0.90) cm with orforglipron. This preserved their previously achieved decrease in waist circumference with an average change from randomization of approximately 1 cm (Extended Data Fig. 2c).
In addition, other cardiometabolic risk factors demonstrated similar preservation of reductions at the end of ATTAIN-MAINTAIN. As an example, in cohort 2 participants subsequently randomized to orforglipron had a mean baseline A1c of 5.6% at the beginning of SURMOUNT-5. At the beginning of ATTAIN-MAINTAIN, after weight reduction with injectables, the A1c improved to a mean of 5.2%. At 52 weeks, the mean A1c remained at 5.2% and retained the improvements in this marker after switching to oral orforglipron. Similar trends were observed in insulin levels, FSG, markers of lipids such as triglycerides and non-HDL, and systolic blood pressure (Extended Data Fig. 4a–e).
Rescue therapy
Starting at week 24, participants on placebo who regained 50% or more of the weight loss achieved during the SURMOUNT-5 trial were initiated on orforglipron as rescue therapy. Participants began taking rescue orforglipron 1 mg orally each day, with dose escalation every 4 weeks until the MTD was achieved as determined by the interactive web response system. For participants taking orforglipron 24 mg, they were allowed to re-escalate to orforglipron 36 mg using the interactive web response system to maintain blinding. Other oral OMMs were not permitted as rescue therapy in the study. In those participants who had ≥50% weight regain in cohort 1 and cohort 2, 39 (65.0%) and 42 (64.6%) received rescue orforglipron therapy in the placebo group, respectively. In those randomized to the orforglipron group, two participants in cohort 1 and one participant in cohort 2 were escalated from a dose of 24 mg to 36 mg of orforglipron. Furthermore, at 52 weeks, only 25 participants (31.3%) from cohort 1 and 12 participants (18.2%) from cohort 2 who were originally randomized to placebo completed treatment without receiving active therapy (either as rescue or other OMMs).
Safety
The proportion of participants reporting any adverse events (AEs) and the number of reported serious adverse events (SAEs) were similar between arms (Table 2; see additional safety data in Extended Data Tables 1 and 2). Across both the cohorts, study drug discontinuations owing to AEs were 4.8% to 7.3% with orforglipron MTD. The most frequently reported AEs with orforglipron were gastrointestinal disorders of nausea, constipation, vomiting or diarrhea. The overall incidence of GI AEs including nausea, vomiting or diarrhea in the first 4 weeks of the trial for both cohorts was 10.5% and 9.5% in the tirzepatide and semaglutide cohorts, respectively. Most GI AEs were mild to moderate in severity, and there were no dose de-escalations within the first 4 weeks when transitioning from injectable therapy directly to 12 mg of orforglipron (Extended Data Fig. 5).
SAEs were reported by three participants in the orforglipron group in cohort 1 and one participant each in the orforglipron and placebo group in cohort 2, accounting for <2% of the total group (Table 2). One case of mild pancreatitis was confirmed through adjudication in the orforglipron treatment group in cohort 1. Among the participants treated with orforglipron in cohort 1, four participants had increased ALT levels greater than or equal to three times the upper limit of normal (ULN) and one participant in cohort 2 and one participant in the placebo group for both cohorts 1 and 2 experienced this elevation in ALT (Extended Data Table 3). In both cohorts 1 and 2, two participants receiving orforglipron had increased AST levels greater than or equal to three times the ULN. In the placebo group, one participant in cohort 2 experienced this elevation (Extended Data Table 3). Of the participants experiencing these aspartate aminotransferase (AST)/alanine aminotransferase (ALT) elevations, one participant in cohort 2 receiving placebo also experienced an increase of twice the ULN for total bilirubin. Overall, no liver safety signals were detected. One death was reported in the orforglipron group in cohort 2 and was not considered related to the study treatment.
Discussion
We present a clinical trial exploring the switch from injectable to oral incretin therapy for the treatment of obesity. In ATTAIN-MAINTAIN, participants treated with orforglipron demonstrated significant and clinically meaningful maintenance of body weight reduction achieved with injectable therapy compared with placebo, with 75% and 79% in the orforglipron group versus 49% and 38% in the placebo group in cohorts 1 and 2, respectively. A key finding of this trial is that participants were better able to maintain the majority of weight loss achieved with injectable therapy when switched to orforglipron compared with placebo. As an initial trial examining switching to oral therapy for maintenance of weight reduction, and in the absence of a widely agreed upon definition or calculation to assess maintenance of weight reduction, several endpoints, including additional sensitivity analyses, were evaluated in this trial regarding maintenance and overall change. We observed that calculating maintenance based on the weight loss achieved in SURMOUNT-5 resulted in relatively high variability due to the limited sample size, which may disproportionately skew the mean and limit clarity and generalizability, particularly given that only 12 participants remained on placebo at week 52 without requiring rescue therapy or other OMMs in the semaglutide-to-placebo group. Thus, additional sensitivity analyses were conducted to provide data including absolute change in mean weight. Mean absolute change in weight may be an important complementary endpoint to facilitate a clearer and fuller understanding of maintenance for the clinical provider. Participants treated with orforglipron demonstrated average reductions in body weight from week 0 to 52 in ATTAIN-MAINTAIN of approximately 5 kg (5%) in cohort 1 and 1 kg (1%) in cohort 2.
Consistent with the orforglipron clinical trial program demonstrating an efficacy and safety profile generally similar to injectable GLP-1 RAs, orforglipron maintained nearly all the weight loss achieved on injectable semaglutide9,14. We hypothesized that patients would experience more weight regain on average when transitioning off high doses of the dual GIP/GLP-1 RA tirzepatide to a GLP-1 RA than when transitioning from a GLP-1 RA to a GLP-1 RA, but further exploration is necessary. A head-to-head clinical trial of injectable tirzepatide versus injectable semaglutide has already demonstrated superior weight loss with tirzepatide12. Even so, most participants transitioning from tirzepatide maintained the majority of their weight loss, particularly compared with placebo, and demonstrated minimal changes in waist circumference as a marker of visceral adiposity, along with sustained improvements in systolic blood pressure, lipid levels and glycemic parameters following weight reduction. For some patients, a small degree of weight regain while maintaining the majority of weight loss achieved with injectable therapy may be clinically acceptable, particularly if switching to a different therapy that has attributes that facilitate long-term persistence on therapy. The individual differences highlight the need for shared decision-making conversations across the entire obesity management journey. An additional finding is that, regardless of the initial intervention, switching to orforglipron resulted in both cohorts ending at the same body weight of 95.9 kg. This finding with orforglipron could suggest that there may be a biological component that controls the disease of obesity at this body weight. Further studies are needed to explore this potential biological control of obesity.
A common misconception among individuals with obesity, as well as some clinicians, is that OMMs can be discontinued after achieving initial weight loss. The approach of stopping medication after intentional weight loss can lead to weight cycling and loss of improvements in cardiometabolic health such as increased insulin resistance or blood pressure, as is seen when individuals stop therapy in other chronic diseases such as hypertension and dyslipidemia3,15,16. So far, injectable OMMs have proven to be highly efficacious and safe for use, but persistence on therapy remains challenging. This trial provides evidence of how to switch to oral OMM therapy and its ability to improve weight loss maintenance and could serve as a potential solution for persistence on therapy for those who wish to stop injectable therapy owing to patient preference, convenience, cost or cold storage requirements.
When the study was originally designed, it was uncertain whether tolerance to high doses of injectable OMMs used in SURMOUNT-5 would confer similar cross-tolerance to an oral nonpeptide agonist like orforglipron. To minimize the dose escalation period, we evaluated transitioning patients directly from injectable therapy to 12 mg of orforglipron (compared with starting doses of 1 mg evaluated in the registration program evaluating participants without recent GLP-1 RA exposure). This transition was generally well tolerated, with fewer than 5% of participants experiencing gastrointestinal AEs and no participants requiring a dose de-escalation in both cohort 1 and cohort 2 during the first 4 weeks of the trial. This tolerability profile raises the question of whether patients could transition directly from injectable incretin therapy to higher doses of orforglipron, potentially minimizing the dose-escalation period required to reach equipotent dosing. Although not explored here, this could be an area of future investigation to further optimize patient convenience and prescribing simplicity.
In our study, participants received rescue orforglipron if they experienced 50% or more weight regain while on placebo starting at 24 weeks post-randomization. The use of rescue orforglipron in this trial was a, patient-centric approach intended to mitigate both the physiological and psychological consequences of weight regain, considering the substantial weight reductions observed in SURMOUNT-5. This patient-centric approach did contribute to complexity when interpreting comparisons to placebo at the 52-week time point. In fact, as expected and demonstrated by results between weeks 24 and 52, the availability of rescue therapy largely prevented further increases in average weight across both cohorts. In both cohorts, the majority of participants who regained ≥50% of their weight reduction were from the placebo arm, which probably contributed to the high study completion rates observed in these arms (81.3% cohort 1, 74.2% cohort 2), despite the increasing availability of OMMs in the USA. This highlights the need for clinicians to educate patients on the importance of persistence on therapy in managing obesity as a chronic condition and to clarify the natural progression of the disease should therapy be halted.
Trial limitations include study sites located only in the USA and a predominantly white study population, although the study includes a more representative US population with a higher Black or African American and Hispanic or Latino population. Additional limitations were the lack of a comparator arm that included continuing injectable OMM and a trial duration of 1 year. Owing to the increasing availability of OMMs, there were participants who discontinued treatment to start available and approved medications, even before the 24 weeks when rescue therapy became an option for placebo. Trial strengths include the randomized, controlled study design, inclusion of healthy lifestyle counseling throughout the trial, and use of rescue orforglipron in case of significant (≥50%) weight regain to limit the potential harm associated with weight regain, although this does not allow for pure placebo versus treatment comparison after week 24. In our study, only 25 participants (31.3%) in cohort 1 and 12 participants (18.2%) in cohort 2 from the placebo arm remained on placebo through week 52 without requiring intervention to manage weight regain. In addition, this trial evaluates switching from injectable OMMs to oral therapy and provides evidence supporting the use of 12 mg of orforglipron as a starting dose after transitioning from injectable therapy.
Once-daily orforglipron minimized weight changes after body weight reduction achieved with tirzepatide or semaglutide for people living with obesity without type 2 diabetes. The results indicate that switching to orforglipron may be an effective approach for maintaining weight loss for those who do not continue injectable therapy.
Methods
Study design
The trial was conducted in compliance with the Declaration of Helsinki and the Good Clinical Practice guidelines of the International Council for Harmonization. The trial protocol was approved by the Advarra central institutional review board. A blind, independent, external committee adjudicated all deaths, pancreatic AEs and cardiovascular events. The completed trial is registered on ClinicalTrials.gov (NCT06584916).
ATTAIN-MAINTAIN consisted of two phase 3b randomized, double-blind, placebo-controlled cohorts conducted at 29 sites in the USA. The trial examined the maintenance of body weight reduction with treatment of orforglipron among participants who previously completed SURMOUNT-5 and received 72 weeks of either tirzepatide (cohort 1) or semaglutide (cohort 2). The tirzepatide and semaglutide treatment groups from the SURMOUNT-5 trial were treated independently and analyzed separately. ATTAIN-MAINTAIN builds upon the findings of the previously published SURMOUNT-5 trial12.
During SURMOUNT-5, participants were randomized to either tirzepatide MTD (10 mg or 15 mg) or semaglutide MTD (1.7 mg or 2.4 mg) with a total weight-loss period of 72 weeks1. After completion of SURMOUNT-5, eligible participants who provided written, informed consent for ATTAIN-MAINTAIN were randomized to either orforglipron or placebo (Extended Data Fig. 6). The study included a screening period of up to 2 weeks after completion of SURMOUNT-5, a 52-week treatment period and a 2-week safety follow-up. A list of study investigators is available in the Supplementary Information.
Participants
Eligible adult participants completed the SURMOUNT-5 trial on study treatment and achieved a body weight reduction of at least 5% at week 72 with either tirzepatide or semaglutide. Exclusion criteria included a diagnosis of diabetes and a BMI of 22 kg/m2 or lower. A complete list of inclusion and exclusion criteria is provided in the Supplementary Information (Protocol Study Population 47). All participants provided signed informed consent before trial participation. Participants were screened and recruited irrespective of sex.
Randomization and blinding
Participants were randomized in a 3:2 ratio to receive once-daily orforglipron (36 mg or MTD of 24 or 36 mg), or placebo, using a computer-generated random sequence from a Lilly interactive web response system. This work reports data on the investigational orforglipron capsule formulation of 1 mg, 3 mg, 6 mg, 12 mg, 24 mg and 36 mg; the doses have been shown as the equivalent to the tablet doses of 0.8 mg, 2.5 mg, 5.5 mg, 9 mg, 14.5 mg and 17.2 mg, respectively, which are approved in the USA13. Randomization was stratified by achievement of plateau at week 72 in SURMOUNT-5, sex and percent weight loss at week 72 of SURMOUNT-5 (<20%, ≥20%). Plateau was defined as a weight change of less than 5% between weeks 60 and 72 in the SURMOUNT-5 study. Study investigators, site staff, clinical monitors and participants were blinded to the study intervention until study completion.
Study interventions
Following randomization, participants initiated blinded orforglipron 12 mg or a matching placebo once daily. The first study intervention dose was ideally administered within 14 days of the last dose of SURMOUNT-5 study drug. Participants randomized to orforglipron increased the dose every 4 weeks until reaching 36 mg or MTD. The maintenance dose of the study intervention was continued for the remainder of the 52-week study. Starting at week 24, participants on placebo who regained 50% or more of the weight loss achieved during the SURMOUNT-5 trial were initiated on orforglipron as rescue therapy. No restrictions were placed on the time of day or food and water intake when taking the study intervention; however, participants were encouraged to take the study intervention at the same time each day. All participants, regardless of treatment assignment, received lifestyle counseling consistent with current guidelines for weight management of a healthy diet and physical activity.
Outcomes
For both cohorts, the primary endpoint was the percent maintenance of body weight reduction in SURMOUNT-5 for participants who achieved a body weight plateau. For each participant, this endpoint is defined as the ratio between the total weight loss achieved between the start of SURMOUNT-5 and the end of ATTAIN-MAINTAIN (week 52) over the total weight loss achieved between the start of SURMOUNT-5 and the baseline of ATTAIN-MAINTAIN (week 0). The key secondary endpoint in plateau participants included the assessment (yes/no) of maintaining at least 80% of body weight reduction. For all participants, the key secondary endpoints included the percent change in body weight from SURMOUNT-5 baseline and percent maintenance of body weight reduction. Additional secondary endpoints include evaluation of maintenance of at least 15% body weight reduction from SURMOUNT-5 baseline for participants who had already lost at least 15% body weight reduction after 72 weeks of tirzepatide or semaglutide treatment, change (in kg) and percent change in body weight from baseline to week 52, and change in waist circumference (in cm) from baseline to week 52. Safety endpoints include the number and incidence of SAEs, treatment-emergent AEs and study intervention discontinuation owing to AEs. Exploratory endpoints included the use of rescue orforglipron for weight regain of 50% or greater of the body weight reduction achieved during SURMOUNT-5, changes in patient-reported outcomes and changes in cardiometabolic parameters. A detailed discussion of retention of improvements in cardiometabolic parameters will be presented in future publications.
Statistical analysis
Sample size
We estimated that a sample size of 150 participants was required for each cohort to ensure that 118 participants reached a plateau in body weight. This sample size provides approximately 90% power to detect a 10% treatment difference for the primary endpoint. This calculation assumed a 20% discontinuation rate and a common standard deviation of 14%, utilizing a two-group t-test with a 5% two-sided significance level.
Statistical methods
The primary hypothesis was that orforglipron 36 mg or MTD was superior to placebo at week 52 for mean percent maintenance of body weight reduction in participants who had reached a body weight plateau in SURMOUNT-5.
Primary and key secondary efficacy endpoints were assessed using either a modified intent-to-treat population who received at least one dose of orforglipron or placebo, excluding participants who were inadvertently enrolled, or a subset of participants who achieved body weight plateau. Two estimands were used in this study: the modified treatment-regimen estimand, considered primary, and the efficacy estimand, considered supportive. All results in this Article are based on the modified treatment-regimen estimand, unless otherwise specified. The modified treatment-regimen estimand evaluated the treatment effect regardless of treatment discontinuation or initiation of prohibited medications. This estimand also assumes that participants who had bariatric surgery or another weight loss procedure or took rescue orforglipron would not have received any additional improvement from their randomized study treatment. For the modified treatment-regimen estimand, the analysis of covariance model was used to analyze continuous measurements at week 52. This analysis adjusted for baseline value, stratification factors (plateau at week 72 in SURMOUNT-5, sex and percent weight loss at week 72 of SURMOUNT-5 (<20%, ≥20%)) and interactions of treatment-by-baseline and treatment-by-stratification factors, incorporating imputed data for missing values at baseline and missing endpoints at week 52. Binary endpoints, such as reaching at least 80% maintenance of body weight reduction at week 52, were analyzed using a logistic regression model, with treatment, stratification factors and continuous baseline value, and interactions of treatment-by-baseline and treatment-by-stratification factors as covariates. The efficacy estimand evaluated the treatment effect assuming that participants had stayed on treatment, had not taken prohibited medications, had not had bariatric surgery or any other weight management procedures and assuming that participants who took rescue orforglipron would not have received any additional improvement from their randomized study treatment. For the efficacy estimand and for continuous endpoints, a maximum-likelihood-based mixed model for repeated measures (MMRM) was used with adjustment for baseline value and stratification factors, considering three-way interactions between treatments, visits and baseline value (or stratification factors). Additional details on statistical methodology can be found in the statistical analysis plan in the Supplementary Information. For the primary and key secondary end points, the overall type I error rate was controlled at a two-sided alpha level of 0.05 within each estimand by means of a graphical testing procedure for each cohort separately.
Safety endpoints were evaluated using the Safety Analysis Set before rescue (SAS-Before Rescue), which included data from all participants who were randomly assigned to the study and had received at least one dose of the study intervention. Data obtained after rescue were excluded. In addition, selected safety endpoints will be evaluated using the Safety Analysis Set Orforglipron (SAS-OFG), which included data after the first dose of orforglipron for participants randomized to orforglipron and data after initiation of rescue orforglipron for participants randomized to placebo. Safety assessments included AEs and SAEs reported throughout the study. The frequency and proportion of participants experiencing AEs and SAEs were summarized descriptively. Categorical comparisons were made using Fisher’s exact test, and risk differences with 95% CIs were provided.
Statistical analyses were computed using R version 4.4.2. Additional statistical methods are available in the Supplementary Information (statistical analysis plan).
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
Lilly provides access to all individual participant data collected during the trial, after anonymization, with the exception of pharmacokinetic or genetic data. Data are available to request 6 months after the indication studied has been approved in the USA and European Union and after primary publication acceptance, whichever is later. No expiration date of data requests is currently set once data are made available. Access is provided after a proposal has been approved by an independent review committee identified for this purpose and after receipt of a signed data sharing agreement. Data and documents, including the study protocol, statistical analysis plan, clinical study report, blank or annotated case report forms, will be provided in a secure data sharing environment. For details on submitting a request, see the instructions provided at www.vivli.org. Source data are provided with this paper.
References
Nadolsky, K. et al. American Association of Clinical Endocrinology Consensus Statement: algorithm for the evaluation and treatment of adults with obesity/adiposity-based chronic disease–2025 update. Endocr. Pract. 31, 1351–1394 (2025).
Gasoyan, H., Pfoh, E. R., Schulte, R., Le, P. & Rothberg, M. B. Early- and later-stage persistence with antiobesity medications: a retrospective cohort study. Obesity 32, 486–493 (2024).
Aronne, L. J. et al. Continued treatment with tirzepatide for maintenance of weight reduction in adults with obesity: the SURMOUNT-4 randomized clinical trial. JAMA 331, 38–48 (2024).
Group AfHiDS. Association of weight loss maintenance and weight regain on 4-year changes in CVD risk factors: the action for health in diabetes (Look AHEAD) clinical trial. Diabetes Care 39, 1345–1355 (2016).
Rosenbaum, M. & Foster, G. Differential mechanisms affecting weight loss and weight loss maintenance. Nat. Metab. 5, 1266–1274 (2023).
Hall, K. D. & Kahan, S. Maintenance of lost weight and long-term management of obesity. Med. Clin. 102, 183–197 (2018).
Aronne, L. J. et al. Describing the weight-reduced state: physiology, behavior, and interventions. Obesity 29, S9–S24 (2021).
Theodorakis, N., Kreouzi, M., Pappas, A. & Nikolaou, M. Beyond calories: individual metabolic and hormonal adaptations driving variability in weight management—a state-of-the-art narrative review. Int. J. Mol. Sci. 25, 13438 (2024).
Horn, D. B. et al. Orforglipron, an oral small-molecule GLP-1 receptor agonist, for the treatment of obesity in people with type 2 diabetes (ATTAIN-2): a phase 3, double-blind, randomised, multicentre, placebo-controlled trial. Lancet 406, 2927–2944 (2025).
Losi, S. et al. The role of patient preferences in adherence to treatment in chronic disease: a narrative review. Drug Target Insights 15, 13 (2021).
Craig, H. et al. Factors that determine patients considering medication for the disease of obesity: an IMI2 SOPHIA study. Int. J. Obesity 49, 397–401 (2025).
Aronne, L. J. et al. Tirzepatide as compared with semaglutide for the treatment of obesity. N. Engl. J. Med. 393, 26–36 (2025).
Ma, X. et al. Pharmacokinetic bioequivalence of orforglipron tablets and capsules in healthy participants with obesity or overweight. Diabetes Obes. Metab. https://doi.org/10.1111/dom.70783 (2026).
Wharton, S. et al. Orforglipron, an oral small-molecule GLP-1 receptor agonist for obesity treatment. N. Engl. J. Med. 393, 1796–1806 (2025).
Wilding, J. P. et al. Weight regain and cardiometabolic effects after withdrawal of semaglutide: the STEP 1 trial extension. Diabetes Obes. Metab. 24, 1553–1564 (2022).
Rubino, D. et al. Effect of continued weekly subcutaneous semaglutide vs placebo on weight loss maintenance in adults with overweight or obesity: the STEP 4 randomized clinical trial. JAMA 325, 1414–1425 (2021).
Acknowledgements
This study was funded by Eli Lilly and Company. We thank all investigators, research team members and, most of all, the study participants. We thank M. Müller, E. Seth and C. Khouli (Eli Lilly and Company) for writing and editorial contributions. The funder of this study was involved with study design, data collection, analysis, interpretation and writing of this report. The authors had full access to the data, and all contributed to and approved this manuscript for publication.
Author information
Authors and Affiliations
Contributions
L.J.A., E.G.V., R.G., C.W.l.R., L.G. and N.X. contributed to the study design. L.J.A., D.B.H., W.H. and N.X. conducted and provided medical oversight during the trial. E.G.V. and C.X. were responsible for the statistical analyses. L.J.A., E.G.V., C.X., D.M.H., L.G. and N.X. are the guarantors of this work and, as such, take responsibility for the integrity of the data and the accuracy of the data analysis. L.J.A., D.B.H., C.W.l.R., A.M.C., W.H., B.H., R.G., C.X., E.G.V., C.J.L., A.R., D.M.H., L.G. and N.X. participated in interpretation of the data and critical review of the manuscript, had full access to all the data in the study and approved of this manuscript to be submitted for publication.
Corresponding author
Ethics declarations
Competing interests
L.J.A. reports receiving grants or personal fees from Altimmune, AstraZeneca, Boehringer Ingelheim, Eli Lilly and Company, ERX, Gelesis, Intellihealth, Jamieson Wellness, Janssen, Novo Nordisk, Optum, Pfizer, Senda Biosciences and Versanis and being a shareholder of ERX Pharmaceuticals, Gelesis, Intellihealth and Jamieson Wellness. D.B.H. reports consulting for Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Novo Nordisk and Zealand and has received institutional research funding from Eli Lilly and Company, KVK Tech, Novo Nordisk and Weight Watchers. C.W.l.R. has acted as a consultant for Arrowhead Pharmaceuticals, AstraZeneca, Boehringer Ingelheim, Currax Pharmaceuticals LLC, Eli Lilly and Company, F. Hoffmann-La Roche AG, Johnson and Johnson, Medtronic and Novo Nordisk. A.M.C. has served on advisory boards to Eli Lilly and Company, Boehringer Ingelheim, Novo Nordisk and Roche, and received travel support from Eli Lilly and Company and Boehringer Ingelheim, honorarium and travel support from Roman Health Ventures Inc., and received grant support, on behalf of Johns Hopkins University, from Eli Lilly and Company. W.H. has acted as a consultant and advisory board member for Eli Lilly and Company. B.H. reports payment or honoraria from Eli Lilly and Company, Novo Nordisk, Merck S.A., AstraZeneca, Boehringer Ingelheim and Abbott Nutrition; travel/meeting support from Novo Nordisk; participation on a Data Safety Monitoring Board or Advisory Board for Eli Lilly, Novo Nordisk, Astra Zeneca, Boehringer Ingelheim and Currax. R.G., C.X., E.G.V., C.J.L., A.R., D.M.H., L.G. and N.X. are employees and shareholders of Eli Lilly and Company.
Peer review
Peer review information
Nature Medicine thanks W. Garvey, Steven Heymsfield and Zilong Yu for their contribution to the peer review of this work. Primary Handling Editor: Ashley Castellanos-Jankiewicz, in collaboration with the Nature Medicine team.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data
Extended Data Fig. 1 Assessment of maintenance of ≥80% body weight reduction achieved.
Key secondary endpoints of assessment of maintenance of ≥80% body weight reduction achieved. Data presented as MBE (SEM). OFG vs. PBO: p-values are for risk difference vs. PBO. A.) Cohort 1 maintenance of ≥80% body weight reduction achieved during SURMOUNT-5. OFG N = 85; Placebo N = 57. Efficacy estimand. B.) Cohort 2 maintenance of ≥80% body weight reduction achieved during SURMOUNT-5. OFG N = 87; Placebo N = 43. Efficacy estimand. Abbreviations: BW = body weight; OFG = orforglipron, PBO = placebo.
Extended Data Fig. 2 Waist circumference change from SURMOUNT-5 to ATTAIN-MAINTAIN.
Sensitivity analysis of waist circumference change from SURMOUNT-5 to ATTAIN-MAINTAIN. A) Cohort 1: Absolute waist circumference from SM-5 to ATTAIN-MAINTAIN. Observed data and efficacy estimand. B) Cohort 1: Mean change in waist circumference from SM-5 to ATTAIN-MAINTAIN. Observed data and efficacy estimand. C) Cohort 2: Absolute waist circumference from SM-5 to ATTAIN-MAINTAIN. Observed data and efficacy estimand. D) Cohort 2: Mean change in waist circumference from SM-5 to ATTAIN-MAINTAIN. Observed data and efficacy estimand. Data presented in line plots are observed mean (SEM). *Data are MBE (SEM) for the mean actual value of waist circumference based on MMRM analysis. Dashes beginning at week 24 include participants eligible for rescue therapy. Data in ATTAIN-MAINTAIN after rescue orforglipron were imputed with worst value observed prior to start of rescue. All other data are MBE (SEM) of mITT population. ICE=intercurrent event; MBE=model-based estimate; mITT=modified intent-to-treat; MMRM=mixed model for repeated measures; MTD=maximum tolerated dose; OFG=orforglipron; PBO=placebo; SEM=standard error of the mean; SEMA=semaglutide, SM-5 = SURMOUNT-5, TZP=tirzepatide.
Extended Data Fig. 3 Cardiometabolic Parameter changes from SURMOUNT-5 to ATTAIN-MAINTAIN in Cohort 1 (Tirzepatide to RCT).
Additional sensitivity analyses of changes in cardiometabolic parameters. Cohort 1 cardiometabolic parameters. Within bar values = number of participants. A.) Lipid parameters mean (SEM) and at Week 52 data MBE (SEM). B.) Systolic blood pressure, mean (SEM) and at Week 52 data as MBE (SEM). C.) HbA1c mean (SEM) and at Week 52 data MBE (SEM). D.) Fasting glucose mean (SEM) and at Week 52 data MBE (SEM). E.) Fasting insulin mean (SEM) and at Week 52 data MBE (SEM). Abbreviations: SM-5 = SURMOUNT-5; ATN-MNTN = ATTAIN-MAINTAIN; HDL=high density lipoprotein; LDL=low density lipoprotein; VLDL=very low density lipoprotein; SBP=systolic blood pressure; SEM=standard error of the mean; MBE=model based estimate.
Extended Data Fig. 4 Cardiometabolic Parameter changes from SURMOUNT-5 to ATTAIN-MAINTAIN in Cohort 2 (Semaglutide to RCT).
Additional sensitivity analysis of changes in cardiometabolic parameters. Cohort 2 cardiometabolic parameters. Within bar values = number of participants. A.) Lipid parameters mean (SEM) and at Week 52 data MBE (SEM). B.) Systolic blood pressure, mean (SEM) and at Week 52 data as MBE (SEM). C.) HbA1c mean (SEM) and at Week 52 data MBE (SEM).D.) Fasting glucose mean (SEM) and at Week 52 data MBE (SEM). E.) Fasting insulin mean (SEM) and at Week 52 data MBE (SEM). Abbreviations: SM-5 = SURMOUNT-5; ATN-MTN = ATTAIN-MAINTAIN; HDL=high density lipoprotein; LDL=low density lipoprotein; VLDL=very low density lipoprotein; SBP=systolic blood pressure; SEM=standard error of the mean; MBE=model based estimate.
Extended Data Fig. 5 Incidence of nausea, vomiting, diarrhea, over time.
Sensitivity analysis of incidence of treatment-emergent nausea, vomiting, diarrhea. Proportions are based on the number of participants at risk. Vomiting includes preferred terms of vomiting and vomiting projectile; diarrhea includes preferred terms of diarrhea and frequent bowel movements; constipation includes preferred terms of constipation, infrequent bowel movements, and feces hard.
Extended Data Fig. 6
Study design and schema.
Supplementary information
Supplementary Information (download PDF )
Supplementary Table 1 (list of investigators), Study Protocol 1 and Statistical Analysis Plan 1.
Source data
Source Data Fig. 2 (download XLSX )
Sensitivity analysis.
Source Data Fig. 3 (download XLSX )
Sensitivity analysis.
Source Data Extended Data Fig./Table 2 (download XLSX )
Sensitivity analysis.
Source Data Extended Data Fig./Table 3 (download XLSX )
Sensitivity analysis.
Source Data Extended Data Fig./Table 4 (download XLSX )
Sensitivity analysis.
Source Data Extended Data Fig./Table 5 (download PDF )
Sensitivity analysis.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/
About this article
Cite this article
Aronne, L.J., Horn, D.B., le Roux, C.W. et al. Orforglipron for maintenance of body weight reduction: the double-blind, randomized phase 3b ATTAIN-MAINTAIN trial. Nat Med (2026). https://doi.org/10.1038/s41591-026-04386-7
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41591-026-04386-7
Facts Only
The ATTAIN-MAINTAIN trial was a double-blind, placebo-controlled study involving 376 participants across 29 sites in the USA.
Participants were previously treated with tirzepatide (cohort 1, N=205) or semaglutide (cohort 2, N=171) in the SURMOUNT-5 study.
Orforglipron is a once-daily oral nonpeptide GLP-1 receptor agonist under investigation for obesity and type 2 diabetes.
Cohort 1 participants maintained 74.7% of body weight reduction with orforglipron vs. 49.2% with placebo at week 52.
Cohort 2 participants maintained 79.3% of body weight reduction with orforglipron vs. 37.6% with placebo at week 52.
Key secondary endpoints, including ≥80% weight loss maintenance, were met in both cohorts.
Common adverse events were gastrointestinal, mostly mild to moderate.
The trial duration was one year, with no comparator arm for continued injectable therapy.
ClinicalTrials.gov registration: NCT06584916.
One death was reported in the orforglipron group in cohort 2, deemed unrelated to treatment.
Rescue therapy with orforglipron was initiated for placebo participants who regained ≥50% of weight loss.
Executive Summary
Full Take
**ACADEMIC MODE**
**Methodology Check:** The study employs a rigorous double-blind, placebo-controlled design with clear primary and secondary endpoints. However, the absence of a comparator arm continuing injectable therapy limits direct comparisons between oral and injectable maintenance strategies. The one-year duration, while sufficient for initial efficacy assessment, may not capture long-term adherence or metabolic adaptations. Sample sizes (N=205 and N=171) are adequate for statistical power but may not fully represent diverse populations, given the predominantly white, female participant demographics.
**Claims vs. Evidence:** The data robustly support orforglipron’s efficacy in maintaining weight loss compared to placebo, with statistically significant differences in both cohorts. However, the abstract’s claim of "safety generally similar to injectable GLP-1 receptor agonists" warrants caution—while gastrointestinal AEs were manageable, the single case of pancreatitis and liver enzyme elevations (though not clinically significant) require further monitoring in larger populations. The framing of "globally scalable" is speculative, as real-world distribution and cost barriers are not addressed.
**Literature Context:** This study extends prior work on GLP-1 agonists by demonstrating the feasibility of switching from injectable to oral therapy without significant weight regain. It aligns with existing evidence on the chronic nature of obesity management but challenges the assumption that injectable therapies are the only viable long-term option. The preservation of cardiometabolic benefits (e.g., HbA1c, waist circumference) is consistent with broader incretin literature.
**Real-World Implications:** If replicated, orforglipron could address key barriers to adherence (e.g., injection aversion, cold chain requirements), potentially improving long-term obesity management. However, its role in clinical practice hinges on cost, accessibility, and long-term safety data beyond one year.
**Bridge Questions:** What would a head-to-head trial comparing orforglipron to continued injectable therapy reveal about efficacy trade-offs? How do patient preferences for oral vs. injectable therapies influence real-world adherence? What metabolic or behavioral mechanisms underlie the observed weight maintenance?
**Counterstrike Scan:** The content aligns with standard clinical trial reporting, with no signs of coordinated influence. The discussion acknowledges limitations transparently, and conclusions are proportionate to the data.