Abstract
Stroke affects 15 million people annually and leaves 5 million permanently disabled. In the chronic phase (>3 months after stroke), patients often experience persistent sensorimotor deficits and altered body representation, yet rehabilitation delivery remains partial and inconsistent, highlighting an unmet clinical need. Immersive technologies and noninvasive neurostimulation offer potential for scalable, intensive rehabilitation, but clinical evidence supporting multimodal approaches and objective outcome assessments remains limited. In this study, we evaluate the feasibility, clinical efficacy and assessment capabilities of a multimodal platform (MultiSensy) integrating virtual reality with synchronous transcutaneous sensory neurostimulation. Thirty-four patients with chronic stroke were enrolled in a combined pilot study (n = 9) and randomized, 33-day-long feasibility study (n = 25), where MultiSensy intervention was evaluated against conventional rehabilitation. Primary endpoints included motor function assessed by Fugl-Meyer Assessment Upper Extremity (FMA-UE) and Action Research Arm Test (ARAT) and self-body representation assessed by the Body Landmark Test. Secondary outcomes included sensory and functional independence evaluation. Continuous kinematic data were collected to derive objective performance markers. Compared to conventional rehabilitation, MultiSensy resulted in greater motor improvement, reflected by higher FMA-UE (13.17 ± 1.30 versus 7.54 ± 1.48; P = 0.01) and ARAT (8.25 ± 1.96 versus 2.44 ± 1.08; P = 0.029) scores. MultiSensy further improved body self-representation and hand tactile acuity. The platform enabled continuous performance monitoring and extraction of objective kinematic markers that tracked rehabilitation progress. These findings pave the way for larger trials and highlight the potential treatment of multiple patients with fewer physiotherapist visits needed or even home-based sensorimotor rehabilitation. ClinicalTrials.gov identifier: NCT06400823.
Similar content being viewed by others
Main
Stroke affects 15 million individuals annually, making it the second-leading cause of death and the third-leading cause of disability worldwide1,2. At the time of hospital admission, stroke survivors face immediate and often severe sensorimotor impairments that affect walking, coordination and speech, resulting in an abrupt loss of autonomy and functional independence3. Despite early rehabilitation efforts to restore cognitive and motor functions, many patients are discharged with persistent deficits that limit their ability to participate in social and professional life4. Notably, clinical evidence demonstrates that recovery extends beyond the acute phase, as patients can significantly improve their clinical status even several months after stroke5,6. At the chronic phase, stroke survivors still experience persistent hemiparetic sensorimotor deficits, such as spasticity, muscle weakness, loss of coordination7 and impaired tactile perception on the affected side8. Moreover, various evidence showed how stroke chronically induces maladaptive plastic changes9,10,11, critically resulting in chronic alterations in movement planning and execution12 and distorted body representation13,14,15,16,17,18 (that is, brain-encoded position and angles of the body19). Namely, for upper-limb impairment, for instance, it was shown15 that patients with chronic stroke misperceive their impaired arm dimensions and have reduced peripersonal space (PPS) (that is, the space in which multisensory stimuli integration is facilitated20,21). However, despite the multidimensionality of stroke deficits across sensory and body representation domains, rehabilitation remains predominantly motor focused22.
In clinical practice, the most common rehabilitation strategy is task-specific training, involving repetitive, goal-directed movements to promote functional recovery and independence. This includes occupational therapy, which targets activities of daily living (ADLs)23, and constraint-induced movement therapy (CIMT)24, which promotes the use of the impaired limb by restricting the unaffected one25. However, task-specific training alone may be insufficient to support full recovery. It could be strengthened by priming techniques26, such as transcranial direct current stimulation or transcutaneous electrical nerve stimulation (TENS), which enhance neural excitability and prepare the brain for relearning, and by augmenting strategies that directly target motor impairments using, for instance, robotic devices. On the other side, functional electrical stimulation (FES) has long been applied in post-stroke upper-limb rehabilitation to restore voluntary movement and prevent disuse-related muscle atrophy27. Several studies have demonstrated clinically meaningful improvements in FMA-UE28 and ARAT29 scores after hybrid FES–robotic30,31. However, although effective for motor reactivation, these systems often lack concurrent sensory feedback, limiting their ability to fully engage sensorimotor integration mechanisms crucial for functional recovery.
Despite their potential, integrated multimodal stroke rehabilitation applications remain rare. Moreover, in real-world practice, rehabilitation type and, more importantly, dosage become highly inconsistent after hospital discharge, leading to tremendous post-acute rehabilitation intensity variability across patients23,32.
To address these challenges, health agencies advocate for innovative multisensory approaches that integrate diverse stroke rehabilitation strategies while delivering high-dosage therapy with minimal supervision, hence reducing the burden on healthcare systems. In this view, virtual reality (VR) can deliver personalized rehabilitation exercises with minimal supervision by medical personnel, accelerating patients’ functional recovery33. Moreover, VR is known to enhance user motivation and engagement through immersive, goal-directed tasks34. This engagement not only improves adherence but also neurophysiologically activates reinforcement-related circuits35,36, including the ventral tegmental area projecting to the motor cortex37,38,39,40, supporting neuroplastic processes critical for motor recovery. Although evidence regarding the efficacy of VR over conventional rehabilitation remains inconclusive41 due to the diversity of VR applications (for example, type, dosage and timing), growing research highlights the benefits of purpose-designed immersive VR42. Integrating tactile cues into immersive visuomotor training provides additional somatosensory information that reinforces sensorimotor coupling34 and offers real-time, task-contingent feedback, an essential component of effective motor relearning in stroke rehabilitation43. In this context, TENS emerges as a noninvasive and cost-effective method for delivering sensory feedback while retraining afferent fibers of the affected limb44,45. TENS has demonstrated efficacy in supporting both sensory and motor recovery, leveraging the critical role of somatosensory input for motor skill acquisition22,46. More crucially, the integration of tactile feedback within immersive VR environments deepens user immersion through synchronous multisensory contingencies47,48,49, a key driver of the ‘body ownership illusion’50 (the sense of inhabiting an alternate body51,52). In principle, this may directly target somatosensory-encoded body representation, hence addressing sensorimotor conflicts and promoting functional recovery12,53. Although recent studies have combined virtual or augmented reality with various forms of noninvasive brain or FES stimulation54,55,56,57, none has yet implemented fully immersive VR integrated with synchronized targeted sensory neurostimulation over multi-week rehabilitation training. Consequently, the potential of immersive VR coupled with peripheral somatosensory stimulation to reinforce body ownership illusions and support motor recovery remains largely unexplored.
Alongside their rehabilitation potential, immersive multimodal systems offer the unique opportunity of continuously tracking participants’ kinematics and body perception status during training (via built-in cameras)58. These objective indicators can be integrated with clinically validated measures, such as the FMA-UE28 and the ARAT29, which evaluate sensorimotor impairment and functional performance in patients with stroke. Combining kinematic and body perception metrics with these tools may offer clinicians a precise and comprehensive profile of a patient’s recovery59, enabling data-driven personalization of rehabilitation strategies.
To these aims, we constructed MultiSensy: a multimodal immersive platform that integrates VR scenarios with congruent targeted sensory neurostimulation (electro-tactile feedback perceived at the site of virtual contact and precisely time synchronous with the interactions with virtual objects) to support sensorimotor rehabilitation and assessment in chronic stroke survivors. The platform was tested on 34 stroke survivors in two stages: a pilot study to assess usability and short-term effects, followed by a randomized feasibility study serving as a proof-of-concept intervention to determine MultiSensy clinical efficacy and impact on motor, body representation and sensory impairments.
Results
Study design and patient demographics
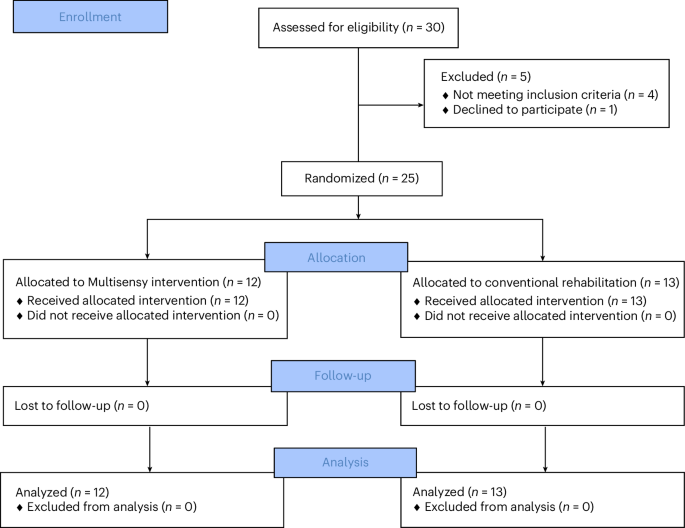
A total of 34 stroke survivors were included in two stages: a pilot study (n = 9) to assess usability and the platform’s short-term effects, followed by a randomized feasibility study (n = 25) to examine its clinical efficacy and rehabilitative impact. Nine participants (one female, eight males; mean age 59 ± 8 years; inclusion and exclusion criteria in Extended Data Table 1) were enrolled in the pilot study. The demographic and clinical characteristics of participants in the pilot phase are summarized in Extended Data Table 2. Twenty-five chronic stroke survivors (nine females, 16 males; mean age 59 ± 10 years) were recruited for the randomized feasibility study (CONSORT diagram in Fig. 1; inclusion/exclusion criteria in Extended Data Table 1). Detailed sample sizes per outcome are provided in Supplementary Table 1.
The recruitment of the randomized feasibility study occurred between April 2024 and April 2025. Participants were randomized into two groups: MultiSensy (n = 12) or conventional rehabilitation (n = 13). Both groups underwent 3 weeks of dose-matched upper-limb rehabilitation, corresponding to 12 sessions (four per week) of active intervention. The MultiSensy group used the immersive neurostimulation platform, completing 6–8 rehabilitation games per session, each lasting at least 4 minutes (Extended Data Fig. 1). The conventional rehabilitation group participated in therapist-supervised sessions, matched in duration and movement types to the MultiSensy sessions (Extended Data Fig. 1). Assessments were conducted at baseline (day 1, T0), midway through the intervention (day 10, T1), at the end (day 19, T2) and at 2-week post-intervention follow-up (day 33, T3).
The demographic (sex and age), clinical (months since stroke, impaired arm, FMA-UE and ARAT) and group allocation data for study participants are summarized in Table 1 (comorbidities are reported in Supplementary Table 2).
Statistical analyses between the two groups were performed to ensure comparability regarding age, months since stroke and FMA-UE and ARAT scores (Supplementary Table 3).
MultiSensy platform and pilot results
MultiSensy is an immersive neurostimulation platform for stroke survivors. It integrates custom immersive VR scenarios with congruent transcutaneous neural stimulation of the median nerve for sensory restoration to offer personalized stroke rehabilitation and assessment (Fig. 2).
On the rehabilitation side, the platform features nine personalized rehabilitation games, each designed to target specific movement and muscular functions (Fig. 2a). The games require the use of the impaired arm exclusively to repetitively perform task-oriented movements, as inspired by constraint-induced therapy (Fig. 2a). The performed movements are combined with task-specific, congruent sensory neurostimulation targeting the median nerve. The electrical stimulation is calibrated to transcutaneously activate sensory fibers in the nerve innervating the thenar region and palmar territories of the thumb, index and middle fingers, which are directly involved in object manipulation during the VR tasks (Fig. 2a). On the assessment side, the platform continuously captures hand and arm poses at a frequency of 50 Hz, generating motion data and kinematic indicators (Fig. 2b). Beyond kinematic assessments, the platform includes two dedicated scenarios for evaluating body perception: the Body Landmark Test60 (Fig. 2c) and the PPS task20 (see ‘Body representation assessment’ section).
The pilot study involved a single-day session where participants performed a shape-tracking task on a vertical plane under two conditions. In the first (MultiSensy), they completed the task within the immersive neurorehabilitation platform (Shapes Game; see ‘Rehabilitation games’ section). In the second, they replicated the task in a real-world scenario using a wall-mounted poster with identical shapes (control) (Fig. 2d). Both conditions lasted 8 minutes, and their order was randomized across participants. Participants evaluated the platform experience with an embodiment (Supplementary Table 4)47,61 and a System Usability Scale (SUS) (Supplementary Table 5)62 questionnaire. Embodiment and control scores (each ranging from −3 to +3) were statistically compared to confirm that participants experienced stronger embodiment sensations than those reflected by the control items63. Participants felt embodied in the platform: embodiment score = 1.64 ± 0.50 (mean ± s.e.m.), control score = −2.04 ± 0.41 (two-sided paired t-test, P < 0.001, Cohenʼs d = 2.64) (Fig. 2e). Participants could intuitively use the platform, with seven of nine rating its usability as ‘excellent’ (SUS > 80.8) and the remaining two as ‘good’ (SUS > 71.1)64 (Fig. 2e). Kinematic analysis of the movements performed in the two conditions is shown in Fig. 2f, highlighting representative kinematic indices (full list in Supplementary Table 6). Velocity (MultiSensy = 0.24 ± 0.02 (m s−1, mean ± s.e.m.), control = 0.17 ± 0.03, P = 0.025) and pronosupination range (MultiSensy = 0.25 ± 0.06, control = 0.09 ± 0.01, P = 0.021) were higher, whereas area error (MultiSensy = 0.37 ± 0.04, control = 0.5 ± 0.04, P = 0.034) was lower in the immersive neurostimulation platform compared to the control condition (Fig. 2f). The smoothness of movement, measured by the number of velocity peaks, showed no significant difference between the two conditions (Fig. 2f). The Body Landmark Test was conducted first at baseline and each time after every experimental condition. The arm length ratio (between perceived and real dimension) improved after the MultiSensy condition (MultiSensy = 0.783 ± 0.039, mean ± s.e.m.) compared to both the baseline (0.571 ± 0.026, P < 0.001) and control (0.499 ± 0.026, P = 0.0004) conditions (Fig. 2g). No significant differences were observed for the hand width ratio (Fig. 2g). Additional indexes and the full statistical analysis are provided in Supplementary Table 7.
Primary outcomes
The primary outcomes of the randomized feasibility trial included motor function assessed by the ARAT and FMA-UE and self body representation assessed by the Body Landmark Test. Single-subject analysis revealed that, in the MultiSensy group, eight of 12 patients achieved a clinically meaningful ARAT improvement (>5.7 (ref. 29)) by T3 compared to three of nine (the other four patients already had 57/57 score) in the conventional rehabilitation group (Fig. 3a,c and Extended Data Table 3).
We next applied a linear mixed-effects model with fixed effects of Group (MultiSensy versus Conventional), Time (T0–T3) and their interaction and random intercepts for participants. The reference levels were Group = Conventional and Time = T0. The mixed model yielded a significant Group × Time interaction (F3,74 = 3.81, P = 0.013), whereas the main effects of Time (F3,74 = 1.49, P = 0.224) and Group (β = 10.06, 95% confidence interval: −5.31 to 25.42, P = 0.196) were not significant. Post hoc comparisons showed significantly greater ARAT improvements in the MultiSensy group at both T2 (MultiSensy = 8.25 ± 1.96, Conventional = 2.44 ± 1.08, P = 0.029) and T3 (MultiSensy = 9.17 ± 2.37, Conventional = 3.11 ± 0.98, P = 0.049) relative to the Conventional group (Fig. 3c and Supplementary Table 8).
For FMA-UE, all 12 patients in the MultiSensy group achieved a clinically meaningful improvement (>5.25 (ref. 65)) by T3, whereas eight of 13 patients in the conventional rehabilitation group showed similar progress (Fig. 3b,d and Extended Data Table 3). The linear mixed-effects model revealed a significant main effect of Time (F3,89 = 20.50, P < 0.001) and a significant Group × Time interaction (F3,89 = 4.86, P = 0.0035), indicating that motor recovery trajectories differed between groups over time. The Group main effect (baseline difference) was not significant (β = −2.72, 95% confidence interval: −14.08 to 8.63, P = 0.635). Post hoc comparisons of baseline-corrected change scores confirmed significantly greater improvements in the MultiSensy group at T3 (MultiSensy = 13.17 ± 1.30, Conventional = 7.54 ± 1.48, P = 0.01) (Fig. 3d and Supplementary Table 8).
For the Body Landmark Test, participants in the MultiSensy group demonstrated improved arm length ratio perception at day 10, T1 (T0 = 0.709 ± 0.039 (mean ± s.e.m.), T1 = 0.916 ± 0.028, P < 0.001), with further improvements at day 19, T2 (T2 = 0.979 ± 0.021, P versus T1 = 0.02) and sustained at day 33, T3 follow-up (0.965 ± 0.027, P versus T0 < 0.001) (Fig. 4a and Extended Data Table 4).
By contrast, no significant improvements were observed for hand perception. Participants in the conventional rehabilitation group showed no improvements in body representation at either the arm or hand level (Fig. 4a and Extended Data Table 5).
Secondary outcomes
Secondary outcomes of the randomized feasibility study included functional independence in ADLs, sensory acuity and PPS. For the Barthel Index, measuring functional independence, four of 12 patients in the MultiSensy group and two of 13 patients in the conventional rehabilitation group showed clinically meaningful improvement by T3 (Extended Data Table 3). However, the linear mixed-effect model revealed no Group × Time interaction (P > 0.05). Participants’ sensory acuity was assessed using the 2-point discrimination (2PD) tactile acuity test (Fig. 4b). At each assessment point, participants were touched repeatedly (n = 40) with either one or two pins and asked to report the number of pins they felt. Accuracy in responses (0−1, where 1 represents 100% accuracy) was used as the tactile acuity outcome (Fig. 4b). Between-group analysis revealed significantly higher 2PD performance improvements at T2 (MultiSensy = 0.162 ± 0.044 (mean ± s.e.m.), conventional = −0.006 ± 0.038, P = 0.008) and T3 (MultiSensy = 0.208 ± 0.046, conventional = 0.030 ± 0.028, P = 0.006) in the MultiSensy group compared to the conventional rehabilitation group (Fig. 4b and Supplementary Table 9). For PPS, reaction times across assessment points and groups are shown in Supplementary Fig. 1. To evaluate PPS changes, a two-way (distances × assessment points) within-subjects ANOVA was conducted. For both groups, the ANOVA revealed no significant interaction effects (MultiSensy P = 0.23, conventional P = 0.37), indicating no multisensory facilitation (reduction in reaction times) at different distances across timepoints.
Safety
No adverse events were reported during either the pilot study or the randomized feasibility study.
Exploratory outcomes
During the rehabilitation games in the immersive neurostimulation platform, we extracted kinematic indicators capturing movement velocity, smoothness and accuracy as well as performance indexes quantifying efficiency and efficacy59 (Fig. 5a and Supplementary Table 10).
MultiSensy games were selected individually by physiotherapists, but two (Shapes and Baseball games) were common to most participants to enable cross-participant comparisons. The Shapes Game involved repetitive hand movements in the frontal plane, and the Baseball Game required hand movements in the transverse plane. Because the conventional rehabilitation group did not use the platform during the trial, its participants completed two sessions of the Shapes Game (frontal plane task), without stimulation, once on the first and once on the last rehabilitation day. This allowed assessment of their overall kinematic improvements during their conventional rehabilitation in the randomized feasibility study.
Representative kinematic indexes from the frontal plane task are shown in Fig. 5b. In the MultiSensy group, participants significantly improved velocity (repeated-measures ANOVA P < 0.001, intervention 1 = 0.19 ± 0.03 (mean ± s.e.m.), intervention 12 = 0.29 ± 0.03, P < 0.001), score rate (repeated-measures ANOVA P < 0.001, intervention 1 = 0.07 ± 0.01, intervention 12 = 0.12 ± 0.02, P < 0.001) and smoothness (repeated-measures ANOVA P < 0.001, intervention 1 = 38.32 ± 3.47, intervention 12 = 28.17 ± 5.44, P < 0.001) throughout the rehabilitation sessions (Fig. 5b). In the conventional rehabilitation group, improvements in velocity (intervention 1 = 0.18 ± 0.03, intervention 12 = 0.21 ± 0.03, P = 0.09) and smoothness (intervention 1 = 52.17 ± 12.80, intervention 12 = 40.61 ± 12.93, P = 0.3) were not significant, whereas score rate increased significantly from intervention 1 to intervention 12 (intervention 1 = 0.07 ± 0.02, intervention 12 = 0.10 ± 0.02, P = 0.03) (Fig. 5b). Between-group analysis revealed significantly higher velocity improvement in the MultiSensy group (P = 0.011) compared to the conventional rehabilitation group (Fig. 5b).
To explore variance in task performances and to investigate the clinical relevance of kinematic indicators, we applied unsupervised machine learning to data from the frontal and transverse plane tasks for the MultiSensy group. Principal component analysis (PCA) revealed that the first principal component (PC1) accounted for 41% of the total variance, and the first eight components together explained 90% of the total variance (Fig. 5c). The weights of PC1 were analyzed to identify the kinematic features that contributed the most to variability in these tasks. In both tasks, features related to efficiency (success rate, task time and hit rate) and smoothness (number of velocity peaks) emerged as key drivers of variance. Notably, none of the features associated with accuracy, speed or efficacy ranked among the top contributors to PC1. PC1 showed a significant correlation with clinical FMA-UE (Pearsonʼs ρ = 0.66, P < 0.001) (Fig. 5c) and ARAT (ρ = 0.60, P < 0.001) scores.
The first eight principal components were further used for k-means clustering, associated with distinct levels of clinical impairment severity (Fig. 5d). Based on their associated clinical score distributions, cluster 1, cluster 2 and cluster 3 corresponded to severe, moderate and mild impairment, respectively. Indeed, patients’ clusters referred to significantly different FMA-UE scores (cluster 1: 28.59 ± 1.84, cluster 2: 37.49 ± 1.24, cluster 3: 50.24 ± 0.64; ANOVA P < 0.001, all post hoc P < 0.001) and ARAT scores (cluster 1: 17.72 ± 3.12, cluster 2: 32.63 ± 2.61, cluster 3: 46.97 ± 0.79; ANOVA P < 0.001, all post hoc P < 0.01) (Fig. 5d). Notably, the differences in mean FMA-UE and ARAT scores across clusters were not only statistically significant but also exceeded the minimal clinically important difference (MCID) for both FMA-UE (5.25 (ref. 65)) and ARAT (5.7 (refs. 29,66)), underscoring their clinical relevance.
Discussion
In this study, we introduced MultiSensy: a multimodal immersive neuro-platform for personalized stroke rehabilitation and assessment. We first conducted a pilot study with nine stroke survivors, demonstrating the platform’s usability and short-term benefits. This was followed by a randomized feasibility study involving 25 patients with chronic stroke, which showed that MultiSensy outperformed conventional physiotherapy across a range of stroke-induced impairments.
Platform usability and short-term effects
Results from the pilot study demonstrated excellent usability, with seven of nine participants reporting high SUS scores, highlighting the platform’s user-friendly, robust and intuitive design. These results are particularly notable, as technical and design-related challenges can hinder the adoption of immersive technologies, particularly among older patients, thereby limiting their rehabilitation potential67,68. The strong sense of embodiment with the virtual avatar further reinforced the ability of the platform to engage users and create an immersive environment. This effect can be attributed to the first-person perspective, the precise mirroring of avatar movements with the patients’ actions and the synchrony between visuomotor interactions and tactile stimulation50,52,69,70. In this pilot trial, participants exhibited improved kinematics in the task performance, with higher velocity and greater forearm pronosupination, likely driven by the platform’s immersive design fostering engagement and motivation71. Pronosupination gains may be attributed to the targeted neurostimulation feature of the game, which encouraged participants to orient the palm toward virtual targets to receive a congruent tactile feedback, thereby promoting repeated forearm rotation, a crucial movement for rehabilitation72. In the Body Landmark Test assessment, our baseline findings aligned with previous literature, confirming that patients with stroke misperceive their impaired arm as shorter15,18. Notably, we observed short-term improvements in arm representation after completion of the task. Although the rehabilitation task duration (8 minutes) exceeded the threshold for inducing body illusions73,74, the debated duration of such effects after the illusion prevents us from conclusively attributing the improvement solely to this factor. Therefore, these results prompted a longitudinal analysis in the planned randomized feasibility study.
Clinical effectiveness of the platform
In the randomized feasibility study, the neuro-immersive intervention demonstrated clinically meaningful improvements at follow-up in ARAT and FMA-UE scores for eight of 12 and for 12 of 12 patients, respectively. Clinically meaningful improvements were determined based on the MCID, defined as an improvement of 5.7 points for ARAT and of 5.25 points for FMA-UE, commonly used as responder endpoints in stroke clinical trials.
The observed improvements at the end of the MultiSensy intervention (T2: ΔARAT > 8, ΔFMA-UE > 9; T3: ΔARAT > 9, ΔFMA-UE > 13) exceeded those reported in most studies on chronic patients using electrical stimulation platforms18,75 or VR-based approaches76,77,78,79,80,81,82 yet remained within the range of a few studies83,84,85, positioning our results among the highest reported for similar interventions. Notably, these outcomes were instead similar to those achieved with immersive VR in subacute patients85,86,87 who are prone to show greater recovery5. When compared to previous FES-based and robotics-based rehabilitation studies, the improvements achieved in the MultiSensy group ranked at the upper end of outcomes reported for hybrid FES−robotic intervention in chronic stroke30,88. Studies combining robotic therapy with electromyography (EMG)-triggered stimulation in subacute patients have shown similar or smaller effects89,90. This suggests that the integration of synchronous multisensory feedback within the immersive MultiSensy protocol may potentiate neuroplastic mechanisms and functional recovery beyond what is typically achieved with conventional robotic or FES-based approaches, even in chronic stroke survivors.
Improvements were also observed in the conventional rehabilitation group, with three and eight participants achieving MCID improvements in ARAT and FMA-UE, respectively. Both groups demonstrated consistent gains in upper-limb motor and functional scores as early as T1, after six rehabilitation sessions. These results likely reflect the often underutilized motor and functional potential in this population, attributed to ‘learned non-use’91,92 of the paretic arm due to prolonged lack of confidence, motivation and access to adequate chronic rehabilitation. As a result, chronic patients may underperform in assessments, not due to irreversible deficits but because they habitually avoid using the affected limb. However, targeted rehabilitation, even over a short period, can rapidly restore this underutilized potential, explaining the early improvements observed in both groups. After evaluating within-group variations in clinical scales, we conducted between-group comparisons, demonstrating that the neuro-platform significantly outperformed conventional rehabilitation. Improvements in ARAT were already significant on day 19 (T2) and sustained on day 33 (T3), whereas FMA-UE improvements reached significance on day 33 (T3). The findings suggest that the developed neuro-platform, which requires minimal supervision during task execution, could match or even surpass the effectiveness of conventional rehabilitation. Conventional approaches often rely heavily on physiotherapy resources, in terms of both personnel and time, making the neuro-platform a potentially more scalable and efficient solution for chronic stroke recovery.
One possible explanation for the greater efficacy observed in the MultiSensy group lies in the role of motivation and reward-based engagement. Unlike conventional therapy, the immersive environment of the platform offered patients real-time, success-contingent feedback and emotionally engaging, goal-directed tasks, conditions known to facilitate reinforcement learning35,36. Motivation and reward are not just psychological bonuses in rehabilitation but, also, biological drivers of motor recovery93,94. These elements are known to engage the brain’s reward system, notably the lateral hypothalamus and dorsal raphe nucleus, which modulate dopaminergic activity in the ventral tegmental area 37,38,95,96. The ventral tegmental area projects to the primary motor cortex, where dopamine release can induce neuroplastic changes essential for motor learning39,40. In our intervention, such reward-driven neuromodulation may have supported the consolidation of motor patterns, contributing to the sustained improvements observed in the MultiSensy group.
Sensory and body representation improvements
Diverse evidence documents sensory impairments after a stroke8,97,98, with tactile acuity frequently employed to assess it18,99. Our findings showed significantly greater improvements in tactile acuity (2PD test) for the MultiSensy group compared to conventional rehabilitation. This outcome is likely reflected in both peripheral and central mechanisms. Although peripheral pathways remain intact in patients with stroke, targeted sensory neurostimulation may still be beneficial by retraining sensory fibers that have become underactive due to patients’ habitual avoidance of using the paretic limb, supporting confidence in their movement. At the same time, sensory neurostimulation may target sensory nerves projecting to brain-damaged areas, hence activating specific neural pathways and promoting functional reorganization100,101,102. On a central level indeed, 2PD is strongly linked to body representation, with clinical evidence showing that changes in somatosensory cortex representation fields are tied to altered thresholds103,104,105,106,107. In this view, these results may then suggest neuroplastic changes induced by the neuro-immersive intervention toward a restored body representation.
This central perspective is further supported by the Body Landmark Test results, which demonstrated improvements in arm representation after just six rehabilitation sessions, further enhanced by the end of the intervention and maintained at the 2-week follow-up. Unlike the pilot phase, these improvements cannot be attributed to short-term VR immersion, as assessments occurred on separate days (2 weeks) from the rehabilitation sessions. Instead, they reflect sustained enhancements in body perception driven by the multimodal intervention. These findings represent a new quantitative perspective on the restorative potential of body ownership illusions in addressing stroke-induced body representation deficits. These deficits, including misjudged body position15, phantom limb sensations17 and anosognosia108 (denial of sensory-motor deficits), have been extensively studied even in other populations109. However, clinical evidence linking improved body representation to multimodal interventions modulating body illusions has been lacking53. Our results address this critical gap, offering evidence that could guide the development of innovative rehabilitation strategies.
Kinematic indicators of recovery
Kinematic analysis showed substantial improvements across most kinematic indexes in the MultiSensy group throughout the rehabilitation period. By contrast, the conventional rehabilitation group showed inconsistent improvements, emphasizing the platform’s greater impact on enhancing task-specific movement execution. These results likely stem from the personalized, task-oriented design of the immersive platform, which enhances engagement and facilitates motor learning. However, we cannot exclude the contribution of habituation effects to the virtual environment. Indeed, participants in the Multisensy group interacted with the platform across multiple sessions, compared to the conventional group, which engaged with it only on the first and last rehabilitation days.
Beyond these findings, it is crucial to recognize the importance of kinematic analysis in complementing clinical scales. Unlike traditional assessments, which are resource intensive, reliant on trained personnel and suffer from inter-examiner variability, kinematic indexes offer an intrinsic advantage: they capture motor performance directly during task execution59,110. This allows real-time, objective monitoring of patient status without disrupting the rehabilitation workflow.
To gather more insight into the extracted kinematic indexes, we performed a PCA on data from the Shapes and Baseball games, which involve repeated movements in the frontal and transverse planes, respectively. The analysis revealed that efficiency and smoothness were the main contributors to inter-participant variability, highlighting their importance in assessing movement quality and differentiating motor performance. These indexes thus emerge as sensitive indicators of motor recovery, providing clinicians with a valuable tool to track patient progress. To establish their clinical validity, we demonstrated significant correlations between the principal components and standard scales (FMA-UE and ARAT), confirming the potential of kinematic metrics as reliable markers of functional status. Moreover, the principal components enabled differentiation between clinically distinct patient clusters, further reinforcing their diagnostic value.
This finding suggests that the platform can infer motor and functional status directly from gameplay data, eliminating the need for frequent, time-intensive clinical evaluations. This capability not only validates the clinical relevance of kinematic assessments but also lays the foundation for future adaptive brain−computer interface (BCI) systems, which could leverage real-time kinematic data to dynamically tailor rehabilitation protocols, enabling fully personalized, home-based, data-driven therapy.
Limitations and future perspectives
This study is a randomized feasibility study serving as a proof-of-concept investigation of a novel therapy. Its efficacy has yet to be fully validated in larger clinical trials. At its current stage, it presents some limitations. First, the follow-up period was limited to 2 weeks, providing only partial insight into the persistence of the observed effects. Hence, extending the follow-up duration will be an objective in future trials. Moreover, although we can exclude differences in rehabilitation as both conditions were matched for therapy duration and exercise content, it remains unclear whether the observed clinical and body representation MultiSensy improvements were primarily driven by the VR-based games, the targeted sensory neurostimulation or their combination. In the present study, we were motivated by targeting both sensorimotor components together; future studies could potentially incorporate single-component conditions (for example, VR-only or sensory neurostimulation-only) to isolate and evaluate the contribution of each modality to the intervention’s outcomes. Regarding the assessments, we acknowledge the presence of occasional missing data from some participants as a limitation. These data gaps arose from practical and logistical constraints inherent to an active inpatient clinical setting. In future larger-scale studies, improved scheduling, staffing and resource allocation will be implemented to further reduce missing data. Overall, although the setup is inherently suitable for home-based rehabilitation, the current trial was conducted in clinical settings. This limits our findings to an initial indication of the platform’s potential for fully remote rehabilitation programs. Follow-up trials will focus on evaluating its effectiveness and feasibility in home-based environments.
Conclusion
Our results show that a digital health platform combining immersive reality and targeted sensory neurostimulation leads to clinically meaningful improvements in motor function, sensory acuity and body representation in patients with chronic stroke. The system enables real-time, objective monitoring of rehabilitation progress through automated kinematic analysis. Building upon this, we envision next-generation digital therapies that are accessible, personalized and scalable for at-home neurorehabilitation.
Methods
Participants
Participants were recruited through the Clinic for Rehabilitation ‘Dr. Miroslav Zotovic’ in Belgrade, Serbia. A total of 34 patients with stroke participated in the study. Nine patients participated in the pilot phase of the study, and 25 patients participated in the randomized feasibility study (see CONSORT diagram; Fig. 1). Biological sex was recorded based on participant self-report. Gender identity was not collected. Participant age and sex are reported in Table 1 and Extended Data Table 2. The study was not designed to assess sex-specific or gender-specific effects; therefore, no sex-based or gender-based subgroup analyses were performed. Participants did not receive financial compensation for participation. Inclusion and exclusion criteria are specified in Extended Data Table 1. All participants read and signed the informed consent form. The experiments were designed and conducted in accordance with the Declaration of Helsinki and received approval from the Ethical Committee of the Clinic for Rehabilitation ‘Dr. Miroslav Zotovic’ (numbers 03-2105/1 and 03-788/2). The randomized feasibility study was registered with ClinicalTrials.gov (NCT06400823).
Multisensory platform
The multisensory platform integrates a wearable immersive reality headset (Meta Quest 2; Meta) with an electrical stimulator (RehaMove3; HASOMED) that delivers 50-Hz biphasic pulses targeting the median nerve (Fig. 2a). For the pilot phase only, we used a VIVE Pro (HTC) headset instead of the Meta Quest 2, equipped with three VIVE trackers positioned on the elbow and wrist of the impaired arm and on the hand of the unimpaired arm. The software platform, developed using Unity, leverages custom C# scripts to create immersive rehabilitation and assessment scenarios and seamlessly controls the electrical stimulator through a custom-developed pipe server, enabling precise stimulation modulation. The system provides a fully customizable library for stroke rehabilitation and assessment, tailored to the specific needs of each patient (Fig. 2a). In all scenarios, participants are fully immersed in a first-person perspective, embodying an avatar. In the pilot phase, hand recognition was achieved using VIVE trackers attached to participants’ limbs to capture movements. For the randomized feasibility study phase, markerless Meta Quest 2 hand recognition modules were seamlessly integrated with custom-developed inverse kinematics to animate the avatar’s shape and pose, precisely mirroring the participant’s movements111. The rehabilitation component of the platform includes nine personalized rehabilitation games, each designed to target specific movement and muscular functions (Fig. 2a). Before performing each game, participants view instructional videos demonstrating the required movements and objectives to ensure proper task execution. The games require the use of the impaired arm exclusively, simulating a virtual constraint-induced therapy setup by prohibiting task completion with the unimpaired hand. Participants interact with the virtual environment through task-oriented movements, completing specific objectives designed to enhance motor recovery (Fig. 2a). The performed movements are complemented by synchronous, targeted TENS of the median nerve in the impaired hand (Fig. 2a). The stimulation is task specific and simulates the interaction of the virtual ‘impaired’ hand with virtual objects. It spreads across the palm and fingers, delivering additional sensory input that enhances the feedback provided by the virtual environment. The intensity of the electrical stimulation is calibrated individually during an initial setup phase. While performing the tasks, participants always see a small black panel displaying their current score, enhancing engagement and motivation to improve their performance. The platform’s assessment component operates both passively and actively. During task performance, it seamlessly captures the pose of the participant’s hands and arms at a refresh rate of 50 Hz, providing continuous motion data (Fig. 2b). In addition to this embedded assessment, the platform includes dedicated scenarios specifically designed to evaluate participant body perception: a VR-based adaptation of the Body Landmark Test60 (Fig. 2c) and a visuo-tactile PPS112 task.
Rehabilitation games
The game design process was clinician driven, based on observations of rehabilitation sessions and therapist inputs to identify key movement patterns and functional tasks. Therapists could select the most appropriate game for each patient, analogous to how they select tasks in conventional therapy. The developed games engaged patients in complex, multi-joint tasks that naturally involve various muscular groups and degrees. However, each game was designed to target a primary movement component, hence pointing at a specific therapeutic goal.
-
1.
Reaching Game: Participants have to reach for virtual balls appearing in front of them. The primary aim is to rehabilitate shoulder flexion and extension. The electrical stimulation is constant, with Gaussian-like pulse-width spikes when the target balls are reached.
-
2.
Shapes Game: Participants have to sequentially catch color-coded balls positioned to form predefined shapes of triangles, hearts or stars. The shapes’ trajectories are positioned on a frontal plane located at arm’s distance from the participant. The game involves all of the shoulder degrees of freedom. Electrical stimulation is constant, with Gaussian-like pulse-width spikes when the balls are reached.
-
3.
Goalkeeper Game: Participants have to sequentially block virtual soccer balls arriving from different angles, simulating the actions of a goalkeeper in a soccer game. The main goal is to rehabilitate shoulder adduction and abduction. The participants receive a constant, 1-second-long stimulation triggered by the contact of the impaired hand with the virtual ball.
-
4.
Baseball Game: Participants have to grasp a virtual baseball bat to hit color-coded balls in sequence. The game focuses on rehabilitating shoulder internal and external rotation (on the transverse plane). The stimulation is constantly applied from the moment the participant grasps the virtual bat, with Gaussian-like pulse-width spikes superimposed upon hitting each ball.
-
5.
Gardening Game: Participants have to use a watering can, using forearm pronation and supination to water virtual plants. This game primarily aims to rehabilitate forearm pronation and supination. The electrical stimulation is applied continuously from when the can is grasped until it is released.
-
6.
Biceps Game: Participants have to perform biceps curl exercises to catch virtual balls. The primary goal is to rehabilitate elbow flexion and extension. Targeted stimulation is delivered as a constant base signal during hand interaction, with Gaussian-like pulse-width spikes upon contact with a ball.
-
7.
Motorbike Game: Participants drive a virtual motorbike, accelerating and decelerating to position it in specific target areas. This game primarily targets wrist palmar flexion and extension. The stimulation is triggered upon grasping the motorbike’s handlebars and modulated based on the motorbike’s velocity.
-
8.
Cleaning Game: Participants have to clean a virtual glass by moving their hand to ‘wipe’ dirty sections. The main aim is to rehabilitate wrist radial and ulnar deviation. The electrical stimulation is triggered upon contact with the glass and sustained during the cleaning motion.
-
9.
Pinch Game: Participants have to pinch and release virtual objects into designated areas. This game focuses on rehabilitating hand opening and closure. The stimulation is triggered upon pinching the object. The pulse width modulates to its maximum following a Gaussian-like profile, stopping when the object is released.
For each game, the experimenter could select a difficulty level ranging from 0 to 1, tailored to the patient’s level of impairment. For example, in the Motorbike Game, setting a difficulty level of 0.5 instead of 1 reduced the required range of wrist palmar flexion and extension needed to accelerate the motorbike.
Study design
The platform testing consisted of two phases: a pilot study to evaluate the platform’s usability and short-term effects on kinematics and body representation, followed by a randomized feasibility trial that serves as a proof-of-concept study to assess the platform’s clinical and rehabilitative impact.
The pilot study involved a single-day protocol where patients completed tasks under two experimental conditions, MultiSensy and control, with the order randomized to minimize bias (Fig. 2d). At first, electrical stimulation was calibrated to determine optimal, individualized parameters using a custom-made Python graphical user interface (GUI). Stimulation was delivered using biphasic, rectangular, charge-balanced pulses at 50 Hz113,114,115.
In the calibration phase, participants received ramps of increasing amplitude (A) and fixed pulse width (PW = 100 μs) and were instructed to report a 5/10 intensity. Electrode placement and stimulation amplitude were adjusted until the sensation was somatotopic, spreading along the median nerve across the palm and fingers. Subsequently, perceptual (minimum, 2/10 intensity) and maximum (below pain, 8/10 intensity) thresholds were determined using ramps of fixed A (the one saved) and increasing PW116,117,118. Participants repeated this process three times, and the mean PW values for the minimum and maximum thresholds were saved for modulating stimulation during rehabilitation games. After the calibration of the stimulation, patients underwent a Body Landmark Test to assess their baseline body perception (Fig. 2d). In the MultiSensy condition, patients performed two consecutive rounds of the Shapes Game within the immersive neurostimulation rehabilitation platform (see the Rehabilitation games section), each lasting 4 minutes (Fig. 2d). During these tasks, synchronous and targeted electrical stimulation of the median nerve was provided. After the tasks, patients repeated the Body Landmark Test and completed an embodiment questionnaire (Supplementary Table 4)47,61 and the SUS (Supplementary Table 5)62 questionnaire (Fig. 2d). In the control condition, patients performed the same Shapes Game movements without VR or electrical stimulation. Instead, posters of predefined dimensions, matching the virtual shapes, were placed on a wall (Fig. 2d). Patients faced the wall and followed the shapes with their impaired hand for two 4-minute sessions. After completing the control task, patients repeated the Body Landmark Test (Fig. 2d). While performing the movements, participants still wore VIVE trackers on their limbs, enabling the collection of kinematic data during the control condition using the same equipment as in the MultiSensy condition.
The rehabilitative impact of the platform was tested in a randomized feasibility study (Extended Data Fig. 1). Patients were randomized into one of two groups: the MultiSensy group or the conventional rehabilitation group. Randomization was conducted using a custom MATLAB script provided by an independent third party to ensure allocation concealment. The required sample size was calculated using G*Power, based on an effect size of 1.38 for immersive VR rehabilitation compared to conventional rehabilitation in improving the FMA-UE28 score in stroke survivors42. The parameters of α = 0.05 and statistical power of 0.90 resulted in a minimum of 12 participants per group. Both groups participated in 3 weeks of dose-matched upper-limb rehabilitation, consisting of 12 1-hour sessions. The original inclusion criterion required an FMA-UE score between 16 and 60. During enrollment, an eligibility-related protocol deviation occurred when clinicians deemed a participant with a score below this threshold suitable for inclusion. The clinicians’ rationale was reviewed by the hospital ethics committee, after which the FMA-UE lower inclusion limit was broadened to 10. In addition, a post hoc sensitivity analysis confirmed that inclusion of these participants did not influence the overall results, thereby supporting the appropriateness of including more severely impaired individuals. In the MultiSensy group, participants completed their rehabilitation within the immersive neurostimulation platform, performing 6–8 different rehabilitation games per session, each lasting a minimum of 4 minutes (Extended Data Fig. 1). Games and difficulty level selection were conducted in collaboration with physiotherapists and tailored to each participant based on their baseline FMA-UE score, ensuring the targeted rehabilitation of specific muscular components (Supplementary Table 11). Before the start of each session, participants underwent a calibration procedure as previously described. For each participant, the electrode locations and the electrical stimulation parameters were tailored to optimize somatotopic accuracy of the referred sensation. On the first day, this preparation and calibration phase required approximately 5–10 minutes; on subsequent sessions, it was reduced to 2–5 minutes, as electrode positions and stimulation settings were fine-tuned based on the saved parameters from the previous session. Participants’ stimulation parameters and location of the reported sensation can be found in Supplementary Table 12 and Supplementary Fig. 2.
In the conventional rehabilitation group, participants underwent therapist-guided upper-limb rehabilitation sessions, matched in duration to those provided by the VR platform (Extended Data Fig. 1). Upper-limb conventional rehabilitation combined physiotherapy and occupational therapy. Physiotherapy focused on maintaining muscle length, reducing spasticity if present and facilitating movement across the three-dimensional space of the impaired arm. It also included exercises to improve motor control, coordination and proprioception of the affected arm. Occupational therapy targeted functional arm activities and daily living tasks. Both physiotherapy and occupational therapy were individually tailored to each participant based on their level of impairment. Only on the first and last session days, participants in the conventional rehabilitation group performed a single Shapes Game (4 minutes) to collect kinematic movement indices at the start and end of the rehabilitation period (see the ‘Machine-learning-powered kinematic analysis of movement’ section).
The assessment timepoints and outcome measures were identical for both groups. Participants underwent assessments at four timepoints: T0 (baseline, before the intervention, day 1), T1 (mid-intervention, after six rehabilitation sessions, day 10), T2 (end of the intervention, day 19) and T3 (follow-up post-intervention, 2 weeks after T2, day 33) (Extended Data Fig. 1). At each assessment, clinical, body perception and sensory measures were collected. Primary outcomes included upper-limb motor and functional recovery, assessed using the FMA-UE28 and the ARAT119, respectively, and self-body representation, assessed using a VR-based adaptation of the Body Landmark Test60. For the secondary outcomes, the Barthel Index120 was used to evaluate the level of assistance required for ADLs; sensory recovery was assessed through tactile acuity using the 2PD test18,99; and PPS was assessed with a visuo-tactile PPS task112.
Clinical motor assessment
All clinical assessments were conducted by therapists blinded to participants’ group allocation. The FMA-UE28 assesses impairments in the upper extremity, wrist, hand and coordination across 33 items. Items are scored on a 3-point scale (0 = cannot perform, 1 = performs partially, 2 = performs fully), with a total score ranging from 0 to 66, reflecting the degree of motor impairment. The ARAT119 evaluates upper-extremity functional performance through 19 items divided into four subtests: grasp, grip, pinch and gross arm movement. Each item is rated on a 4-point ordinal scale: 3 = performs normally, 2 = completes with difficulty, 1 = performs partially, 0 = cannot perform. To assess the degree of assistance required for ADLs, the Barthel Index120 was used. It measures the time and physical assistance needed for specific ADLs with a total score ranging from 0 to 100, where higher scores indicate greater independence. Each of the 10 ADL items is rated as 0 = unable, 5 = needs help (verbal, physical or assistive aid) or 10 = independent.
Body representation assessment
Body representation was tested via a VR-based adaptation of the Body Landmark Test60 and a visuo-tactile PPS task112. The Body Landmark Test assesses short-term body representation by encoding the current position and angles of the upper limb19. In the original version60, participants sat with their forearm fixed on a table, hidden from view by a wooden frame, and verbally guided the experimenter to move a marker to align with the perceived position of five anatomical landmarks: index finger, annular finger, radius styloid, ulnar styloid and olecranon. Discrepancies between the actual (recorded while blindfolded) and perceived positions of these landmarks were measured. In our VR-based setup, participants positioned their forearm on a table with a virtual black panel displayed above the arm. They verbally guided the experimenter to move a laser pointer over the virtual panel to align with the perceived positions of the landmarks. For each participant, this was repeated five times for each of the landmarks (25 repetitions in total, randomized), and the average position of each landmark was extracted. From these data, four indices were calculated for both actual and perceived landmark positions: Arm Length (olecranon to the midpoint of radius styloid and ulnar styloid), Arm Width (distance between radius styloid and ulnar styloid), Hand Length (midpoint of radius styloid and ulnar styloid to the midpoint of index finger and annular finger) and Hand Width (distance between index finger and annular finger). Ratios of perceived to actual dimensions for each index were extracted, with a ratio of 1 indicating a perfect match. The validity of the VR-based Body Landmark Test system was assessed in a validation study with 16 healthy controls using both the Meta Quest 2 and HTC VIVE Pro headsets. The study revealed minor systematic errors (<2 cm), which were significantly lower than the improvements observed during the trial for the indexes of interest (Extended Data Fig. 2).
PPS could be defined as ‘the space immediately surrounding our bodies’121, ‘where human–environment interactions take place through multisensory integration’20. It is well established that reaction times to stimuli (for example, vision and touch) become faster when these stimuli occur within the boundaries of the PPS (that is, closer to the body). The virtual PPS testing scenario involved participants seated at a table with their impaired hand positioned on a VR-based marker 0.5 m from their head. A virtual ball appeared 1.5 m away from the marker and moved toward it at a speed of 0.75 m s−1. During trials, 100-ms electrical pulses were randomly delivered to the impaired hand at five fixed distances (0.93 m, 0.71 m, 0.5 m, 0.27 m and 0 m from the marker). Participants were instructed to press a trigger on the VR-based controller (using the unimpaired hand) as soon as they felt the stimulation. Each distance was tested across 15 trials (75 experimental trials in total), along with 25 baseline trials (electrical stimulation only, no ball) and 15 catch trials (no stimulation despite the looming ball). Reaction times to the electrical stimulation were recorded for all trials.
Sensory assessment
To assess sensory recovery after the intervention, tactile acuity was assessed with the 2PD test122. Participants were touched on the palm of the hand with either one or two pins at a fixed distance and asked to identify the number of pins. At T0, the pin distance was individually calibrated by repeatedly increasing the pin distance from 2 mm, with 2-mm increments. For each distance, participants were touched six times with both pins and asked to identify whether they felt one or two pins. The smallest distance at which participants correctly identified at least three out of six stimuli was selected, along with the next larger distance (2 mm longer). At these two distances, participants were touched 20 times each (n = 40) with either one or two pins, and the percentage of correct responses was recorded as the outcome measure. At subsequent assessment timepoints (T1, T2 and T3), the exact same distances calibrated at T0 were used for testing.
Machine-learning-powered kinematic analysis of movement
While participants performed rehabilitation tasks within the immersive neurostimulation platform, the system seamlessly collected hand and arm pose data (positions and angles) at a fixed rate of 50 Hz. These data were used to extract kinematic indices of movement for each game, providing an objective assessment of motor recovery across sessions. Kinematic indicators were extracted and grouped accordingly to ref. 59 in efficiency, efficacy, accuracy, smoothness and speed indicators (Supplementary Table 10). Of these, the indicators from the Shapes and Baseball games were analyzed using machine learning techniques. Missing data for specific days were handled using Iterative Imputer (max_iter = 10). First, PCA was performed to determine the number of components needed to explain the variance in the data. The correlation between PC1 and clinical scales, specifically FMA-UE and ARAT, was computed to evaluate whether the kinematic indices were linked to patients’ clinical status. Next, the principal components explaining up to 90% of the variance were used in an unsupervised k-means clustering analysis to test whether participants could be stratified into clinically meaningful levels of disability using kinematic variables alone. In this analysis, each data point corresponded to a single kinematic observation from one patient during one therapy session. Because FMA-UE and ARAT were assessed at only three timepoints (T0, before session 1; T1, after session 6; and T2, after session 12), intermediate values were linearly interpolated between these assessments to assign each therapy session a corresponding clinical status. Finally, we tested whether the resulting kinematic clusters corresponded to significantly different levels of motor impairment, as quantified by FMA-UE and ARAT scores.
Statistical analysis
For all analyses, parametric or nonparametric tests were selected based on data normality, as assessed by the Kolmogorov−Smirnov test. Clinical outcomes, including improvements in FMA-UE, ARAT and Barthel Index, were initially evaluated against predefined thresholds for clinically meaningful improvements rather than statistical tests. Clinical meaningful thresholds were set at 5.25 points for FMUE65, at 5.7 points for ARAT29 and at 9.25 points for the Barthel Index123. Group and time effects on FMA-UE, ARAT and Barthel Index were analyzed using a linear mixed-effects model with fixed effects of Group (MultiSensy versus Conventional), Time (T0–T3) and their interaction and random intercepts for participants. The reference levels were Group = Conventional and Time = T0. Post hoc comparisons of baseline-corrected change scores (for example, ΔFMA-UE) were performed using either parametric t-tests or nonparametric Mann−Whitney tests, depending on data normality, to evaluate between-group differences at each timepoint. Additionally, a secondary analysis was conducted to assess whether treatment efficacy varied with participant chronicity. An ANCOVA was fitted, including FMA-UE, treatment group, months since stroke and their interactions as parameters. Detailed results are provided in the supplementary materials.
Similarly, between-group comparisons for 2PD improvements were conducted using the same statistical approach. Body Landmark Test indices were analyzed using repeated-measures ANOVA (or Friedman tests, depending on normality) to evaluate variations between assessment points among groups. Least significant difference (LSD) post hoc tests were applied for multiple comparisons where appropriate. For PPS changes analysis among groups, a two-factor (5 distances × 4 assessment timepoints) within-subjects ANOVA was performed to identify significant interaction effects, indicating multisensory facilitation (reduction in reaction times) occurring at different distances depending on the timepoints. In cases where a significant interaction was observed, PPS was calculated for each timepoint as the distance at which reaction times became significantly faster than baseline (paired t-test or Wilcoxon test, depending on normality). For the kinematic analysis, single indicators were compared across days within the MultiSensy group using repeated-measures ANOVA (or Friedman test, depending on normality), followed by LSD post hoc tests. In the conventional rehabilitation group, paired t-tests (or Wilcoxon tests, depending on normality) were used to compare intervention 1 and intervention 12. Between-group improvement analyses were conducted using independent t-tests (or Mann−Whitney tests, depending on normality). Correlations between kinematic principal components and FMA-UE/ARAT scores were analyzed using Pearson’s correlation. k-means identified clusters were compared using ANOVA, followed by LSD post hoc tests for multiple comparisons. For each analysis, all available valid observations were used for descriptive summaries. For statistical tests, missing data were handled according to the respective model used. Data were analyzed using custom scripts written in MATLAB (R2024a; MathWorks) and Python (version 3.13).
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
The data that support the findings of this study are available on Zenodo (https://doi.org/10.5281/zenodo.16043228 (ref. 124)). The study protocol is included in the Supplementary Information.
Code availability
The custom code used to process and analyze the data and generate the figures is available on Zenodo (https://doi.org/10.5281/zenodo.16043228 (ref. 124)).
References
Katan, M. & Luft, A. Global burden of stroke. Semin. Neurol. 38, 208–211 (2018.
Pacheco-Barrios, K. et al. Burden of stroke and population-attributable fractions of risk factors in Latin America and the Caribbean. J. Am. Heart Assoc.11, e027044 (2022).
Lawrence, E. S. et al. Estimates of the prevalence of acute stroke impairments and disability in a multiethnic population. Stroke 32, 1279–1284 (2001).
Brosseau, L., Philippe, P., Potvin, L. & Boulanger, Y.-L. Post-stroke inpatient rehabilitation. I. Predicting length of stay. Am. J. Phys. Med. Rehabil. 75, 422−430 (1996).
Langhorne, P., Bernhardt, J. & Kwakkel, G. Stroke rehabilitation. Lancet 377, 1693–1702 (2011).
Teasell, R. et al. Time to rethink long-term rehabilitation management of stroke patients. Top. Stroke Rehabil. 19, 457–462 (2012).
Ingram, L. A., Butler, A. A., Brodie, M. A., Lord, S. R. & Gandevia, S. C. Quantifying upper limb motor impairment in chronic stroke: a physiological profiling approach. J. Appl. Physiol. (1985) 131, 949–965 (2021).
Doyle, S., Bennett, S., Fasoli, S. E. & McKenna, K. T. Interventions for sensory impairment in the upper limb after stroke. Cochrane Database Syst. Rev. 2010, CD006331 (2010).
Takeuchi, N. & Izumi, S.-I. Maladaptive plasticity for motor recovery after stroke: mechanisms and approaches. Neural Plast. 2012, 359728 (2012).
Dancause, N. & Nudo, R. J. Shaping plasticity to enhance recovery after injury. Prog. Brain Res. 192, 273–295 (2011).
Chen, H., Epstein, J. & Stern, E. Neural plasticity after acquired brain injury: evidence from functional neuroimaging. PM R 2, S306–S312 (2010).
Matamala-Gomez, M. et al. Changing body representation through full body ownership illusions might foster motor rehabilitation outcome in patients with stroke. Front. Psychol. 11, 1962 (2020).
Berlucchi, G. & Aglioti, S. M. The body in the brain revisited. Exp. Brain Res. 200, 25–35 (2010).
Mastria, G. et al. Body ownership alterations in stroke emerge from reduced proprioceptive precision and damage to the frontoparietal network. Med 6, 100536 (2025).
Bassolino, M. et al. Body and peripersonal space representations in chronic stroke patients with upper limb motor deficits. Brain Commun. 4, fcac179 (2022).
Connell, L. A., Lincoln, N. B. & Radford, K. A. Somatosensory impairment after stroke: frequency of different deficits and their recovery. Clin. Rehabil. 22, 758–767 (2008).
Bakheit, A. M. O. & Roundhill, S. Supernumerary phantom limb after stroke. Postgrad. Med. J. 81, e2 (2005).
Crema, A. et al. Neuromuscular electrical stimulation restores upper limb sensory-motor functions and body representations in chronic stroke survivors. Med 3, 58–74 (2022).
de Vignemont, F. Body schema and body image—pros and cons. Neuropsychologia 48, 669–680 (2010).
Serino, A. et al. Peripersonal space: an index of multisensory body–environment interactions in real, virtual, and mixed realities. Front. ICT https://doi.org/10.3389/fict.2017.00031 (2018).
Serino, A. Peripersonal space (PPS) as a multisensory interface between the individual and the environment, defining the space of the self. Neurosci. Biobehav. Rev. 99, 138–159 (2019).
Edwards, L. L., King, E. M., Buetefisch, C. M. & Borich, M. R. Putting the ‘sensory’ into sensorimotor control: the role of sensorimotor integration in goal-directed hand movements after stroke. Front. Integr. Neurosci. 13, 16 (2019).
Winstein, C. J. et al. Guidelines for adult stroke rehabilitation and recovery: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 47, e98–e169 (2016).
Kwakkel, G., Veerbeek, J. M., van Wegen, E. E. H. & Wolf, S. L. Constraint-induced movement therapy after stroke. Lancet Neurol. 14, 224–234 (2015).
Wolf, S. L. et al. Effect of constraint-induced movement therapy on upper extremity function 3 to 9 months after stroke: the EXCITE randomized clinical trial. JAMA 296, 2095–2104 (2006).
da Silva, E. S. M. et al. The effect of priming on outcomes of task-oriented training for the upper extremity in chronic stroke: a systematic review and meta-analysis. Neurorehabil. Neural Repair 34, 479–504 (2020).
Marquez-Chin, C. & Popovic, M. R. Functional electrical stimulation therapy for restoration of motor function after spinal cord injury and stroke: a review. Biomed. Eng. Online 19, 34 (2020).
Fugl-Meyer, A. R., Jääskö, L., Leyman, I., Olsson, S. & Steglind, S. The post-stroke hemiplegic patient. 1. a method for evaluation of physical performance. Scand. J. Rehabil. Med. 7, 13–31 (1975).
Lang, C. E., Wagner, J. M., Dromerick, A. W. & Edwards, D. F. Measurement of upper-extremity function early after stroke: properties of the Action Research Arm Test. Arch. Phys. Med. Rehabil. 87, 1605–1610 (2006).
Ambrosini, E. et al. A robotic system with EMG-triggered functional eletrical stimulation for restoring arm functions in stroke survivors. Neurorehabil. Neural Repair 35, 334–345 (2021).
Popović, D. B. Chapter 20 - Hybrid FES-robot devices for training of activities of daily living. In Rehabilitation Robotics (eds Colombo, R. & Sanguineti, V.) 277–287 (Academic Press, 2018).
Allison, R. et al. The effectiveness of various models of primary care-based follow-up after stroke: a systematic review. Prim. Health Care Res. Dev. 12, 214–222 (2011).
Chen, Y. et al. Home-based technologies for stroke rehabilitation: a systematic review. Int. J. Med. Inform. 123, 11–22 (2019).
Perez-Marcos, D. Virtual reality experiences, embodiment, videogames and their dimensions in neurorehabilitation. J. Neuroeng. Rehabil. 15, 113 (2018).
Zhao, J., Zhang, G. & Xu, D. The effect of reward on motor learning: different stage, different effect. Front. Hum. Neurosci. 18, 1381935 (2024).
Robertson, I. H. The neglected role of reward in rehabilitation. J. Neurol. Neurosurg. Psychiatry 84, 363 (2013).
Tyree, S. M. & de Lecea, L. Lateral hypothalamic control of the ventral tegmental area: reward evaluation and the driving of motivated behavior. Front. Syst. Neurosci. 11, 50 (2017).
Nieh, E. H. et al. Inhibitory input from the lateral hypothalamus to the ventral tegmental area disinhibits dopamine neurons and promotes behavioral activation. Neuron 90, 1286–1298 (2016).
Kunori, N., Kajiwara, R. & Takashima, I. Voltage-sensitive dye imaging of primary motor cortex activity produced by ventral tegmental area stimulation. J. Neurosci. 34, 8894–8903 (2014).
Hosp, J. A., Pekanovic, A., Rioult-Pedotti, M. S. & Luft, A. R. Dopaminergic projections from midbrain to primary motor cortex mediate motor skill learning. J. Neurosci. 31, 2481–2487 (2011).
Laver, K. E. et al. Virtual reality for stroke rehabilitation. Cochrane Database Syst. Rev. 11, CD008349 (2017).
Hao, J., He, Z., Yu, X. & Remis, A. Comparison of immersive and non-immersive virtual reality for upper extremity functional recovery in patients with stroke: a systematic review and network meta-analysis. Neurol. Sci. 44, 2679–2697 (2023).
Maier, M., Ballester, B. R. & Verschure, P. F. M. J. Principles of neurorehabilitation after stroke based on motor learning and brain plasticity mechanisms. Front. Syst. Neurosci. 13, 74 (2019).
Bucciarelli, V. et al. Multiparametric non-linear TENS modulation to integrate intuitive sensory feedback. J. Neural Eng. 20, 036026 (2023).
Gozzi, N. et al. Wearable non-invasive neuroprosthesis for targeted sensory restoration in neuropathy. Nat. Commun. 15, 10840 (2024).
Bolognini, N., Russo, C. & Edwards, D. J. The sensory side of post-stroke motor rehabilitation. Restor. Neurol. Neurosci. 34, 571–586 (2016).
Preatoni, G., Dell’Eva, F., Valle, G., Pedrocchi, A. & Raspopovic, S. Reshaping the full body illusion through visuo-electro-tactile sensations. PLoS ONE 18, e0280628 (2023).
Aurucci, G. V., Preatoni, G., Damiani, A. & Raspopovic, S. Brain-computer interface to deliver individualized multisensory intervention for neuropathic pain. Neurotherapeutics20, 1316−1329(2023).
Aurucci, G. V. et al. Targeted neural stimulation congruent with immersive reality decreases neuropathic pain. Brain Stimul. 18, 1671–1674 (2025).
Maselli, A. & Slater, M. The building blocks of the full body ownership illusion. Front. Hum. Neurosci. 7, 83 (2013).
Lenggenhager, B., Tadi, T., Metzinger, T. & Blanke, O. Video ergo sum: manipulating bodily self-consciousness. Science 317, 1096–1099 (2007).
Kilteni, K., Maselli, A., Kording, K. P. & Slater, M. Over my fake body: body ownership illusions for studying the multisensory basis of own-body perception. Front. Hum. Neurosci. 9, 141 (2015).
Ventura, S., Marchetti, P., Baños, R. & Tessari, A. Body ownership illusion through virtual reality as modulator variable for limbs rehabilitation after stroke: a systematic review. Virtual Reality 27, 2481–2492 (2023).
Zhang, N., Wang, H., Wang, H. & Qie, S. Impact of the combination of virtual reality and noninvasive brain stimulation on the upper limb motor function of stroke patients: a systematic review and meta-analysis. J. Neuroeng. Rehabil. 21, 179 (2024).
Shell, A. K., Pena, A. E., Abbas, J. J. & Jung, R. Novel neurostimulation-based haptic feedback platform for grasp interactions with virtual objects. Front. Virtual Real. https://doi.org/10.3389/frvir.2022.910379 (2022).
Seitz, S. et al. Effect of concurrent action observation, peripheral nerve stimulation and motor imagery on dexterity in patients after stroke: a pilot study. Sci. Rep. 14, 14858 (2024).
Cui, Y., Cong, F., Zeng, M. & Wang, J. Effects and mechanisms of synchronous virtual reality action observation and electrical stimulation on upper extremity motor function and activities of daily living in patients with stroke: a protocol for a randomized controlled trial. Front. Neurol. 16, 1499178 (2025).
Abdlkarim, D. et al. A methodological framework to assess the accuracy of virtual reality hand-tracking systems: a case study with the Meta Quest 2. Behav. Res. 56, 1052–1063 (2024).
Schwarz, A., Kanzler, C. M., Lambercy, O., Luft, A. R. & Veerbeek, J. M. Systematic review on kinematic assessments of upper limb movements after stroke. Stroke 50, 718–727 (2019).
Sorrentino, G. et al. How ageing shapes body and space representations: a comparison study between healthy young and older adults. Cortex 136, 56–76 (2021).
Gonzalez-Franco, M. & Peck, T. C. Avatar embodiment. Towards a standardized questionnaire. Front. Robot. AI 5, 74 (2018).
Brooke, J. SUS: a quick and dirty usability scale. In Usability Evaluation in Industry (eds Jordan, P. W., Thomas, B., McClelland, I. L. & Weerdmeester, B.) (CRC Press, 1996).
Risso, G. et al. Multisensory stimulation decreases phantom limb distortions and is optimally integrated. iScience 25, 104129 (2022).
Sauro, J. 5 ways to interpret a SUS score. https://measuringu.com/interpret-sus-score/ (2018).
Page, S. J., Fulk, G. D. & Boyne, P. Clinically important differences for the upper-extremity Fugl-Meyer Scale in people with minimal to moderate impairment due to chronic stroke. Phys. Ther. 92, 791−798 (2012).
van der Lee, J. H., Beckerman, H., Lankhorst, G. J. & Bouter, L. M. The responsiveness of the Action Research Arm test and the Fugl-Meyer Assessment scale in chronic stroke patients. J. Rehabil. Med. 33, 110–113 (2001).
Zanatta, F., Giardini, A., Pierobon, A., D’Addario, M. & Steca, P. A systematic review on the usability of robotic and virtual reality devices in neuromotor rehabilitation: patients’ and healthcare professionals’ perspective. BMC Health Serv. Res. 22, 523 (2022).
Lloréns, R., Noé, E., Colomer, C. & Alcañiz, M. Effectiveness, usability, and cost-benefit of a virtual reality–based telerehabilitation program for balance recovery after stroke: a randomized controlled trial. Arch. Phys. Med. Rehabil. 96, 418–425.e2 (2015).
Pozeg, P. et al. Virtual reality improves embodiment and neuropathic pain caused by spinal cord injury. Neurology 89, 1894–1903 (2017).
Pyasik, M., Ciorli, T. & Pia, L. Full body illusion and cognition: a systematic review of the literature. Neurosci. Biobehav. Rev. 143, 104926 (2022).
Ceradini, M., Losanno, E., Micera, S., Bandini, A. & Orlandi, S. Immersive VR for upper-extremity rehabilitation in patients with neurological disorders: a scoping review. J. Neuroeng. Rehabil. 21, 75 (2024).
Lambercy, O. et al. Effects of a robot-assisted training of grasp and pronation/supination in chronic stroke: a pilot study. J. Neuroeng. Rehabil. 8, 63 (2011).
Kondo, R. & Sugimoto, M. Effects of virtual hands and feet on the onset time and duration of illusory body ownership. Sci. Rep. 12, 11802 (2022).
Keenaghan, S. et al. My body until proven otherwise: exploring the time course of the full body illusion. Conscious. Cogn. 78, 102882 (2020).
Carda, S. et al. Electrically assisted movement therapy in chronic stroke patients with severe upper limb paresis: a pilot, single-blind, randomized crossover study. Arch. Phys. Med. Rehabil. 98, 1628–1635 (2017).
Perez-Marcos, D. et al. Increasing upper limb training intensity in chronic stroke using embodied virtual reality: a pilot study. J. Neuroeng. Rehabil. 14, 119 (2017).
Turolla, A. et al. Virtual reality for the rehabilitation of the upper limb motor function after stroke: a prospective controlled trial. J. Neuroeng, Rehabil. 10, 85 (2013).
Cameirão, M. S., Badia, S. B. I., Duarte, E., Frisoli, A. & Verschure, P. F. M. J. The combined impact of virtual reality neurorehabilitation and its interfaces on upper extremity functional recovery in patients with chronic stroke. Stroke 43, 2720–2728 (2012).
Huang, C.-Y. et al. Effects of virtual reality-based motor control training on inflammation, oxidative stress, neuroplasticity and upper limb motor function in patients with chronic stroke: a randomized controlled trial. BMC Neurol. 22, 21 (2022).
Kottink, A. I. R., Prange, G. B., Krabben, T., Rietman, J. S. & Buurke, J. H. Gaming and conventional exercises for improvement of arm function after stroke: a randomized controlled pilot study. Games Health J. 3, 184–191 (2014).
Oh, Y.-B. et al. Efficacy of virtual reality combined with real instrument training for patients with stroke: a randomized controlled trial. Arch. Phys. Med. Rehabil. 100, 1400–1408 (2019).
Sebastián-Romagosa, M. et al. Brain computer interface treatment for motor rehabilitation of upper extremity of stroke patients—a feasibility study. Front. Neurosci. 14, 591435 (2020).
Henrique, P. P. B., Colussi, E. L. & Marchi, A. C. B. D. Effects of exergame on patients’ balance and upper limb motor function after stroke: a randomized controlled trial. J. Stroke Cerebrovasc. Dis. 28, 2351–2357 (2019).
Ögün, M. N. et al. Effect of leap motion-based 3D immersive virtual reality usage on upper extremity function in ischemic stroke patients. Arq. Neuropsiquiatr. 77, 681–688 (2019).
Miclaus, R. et al. Non-immersive virtual reality for post-stroke upper extremity rehabilitation: a small cohort randomized trial. Brain Sci. 10, 655 (2020).
Lülsdorff, K. et al. Neurorehabilitation of the upper extremity – immersive virtual reality vs. electromechanically assisted training. A comparative study. Front. Neurol. 14, 1290637 (2023).
Shin, S. et al. A smart glove digital system promotes restoration of upper limb motor function and enhances cortical hemodynamic changes in subacute stroke patients with mild to moderate weakness: a randomized controlled trial. J. Clin. Med. 11, 7343 (2022).
Perini, G. et al. Sequentially applied myoelectrically controlled FES in a task-oriented approach and robotic therapy for the recovery of upper limb in post-stroke patients: a randomized controlled pilot study. Technol. Health Care 29, 419–429 (2021).
Yang, S.-W. et al. Effect of 3-dimensional robotic therapy combined with electromyography-triggered neuromuscular electrical stimulation on upper limb function and cerebral cortex activation in stroke patients: a randomized controlled trial. Bioengineering 11, 12 (2023).
Aprile, I. et al. Upper limb robotic rehabilitation after stroke: a multicenter, randomized clinical trial. J. Neurol. Phys. Ther. 44, 3–14 (2020).
Ballester, B. R. et al. Counteracting learned non-use in chronic stroke patients with reinforcement-induced movement therapy. J. Neuroeng. Rehabil. 13, 74 (2016).
Taub, E., Uswatte, G., Mark, V. W. & Morris, D. M. M. The learned nonuse phenomenon: implications for rehabilitation. Eura. Medicophys. 42, 241–256 (2006).
Wood, A. N. New roles for dopamine in motor skill acquisition: lessons from primates, rodents, and songbirds. J. Neurophysiol. 125, 2361–2374 (2021).
Vitrac, C., Nallet-Khosrofian, L., Iijima, M., Rioult-Pedotti, M.-S. & Luft, A. Endogenous dopamine transmission is crucial for motor skill recovery after stroke. IBRO Neurosci. Rep. 13, 15–21 (2022).
Wang, H.-L. et al. Dorsal raphe dual serotonin-glutamate neurons drive reward by establishing excitatory synapses on VTA mesoaccumbens dopamine neurons. Cell Rep. 26, 1128–1142.e7 (2019).
Qi, J. et al. A glutamatergic reward input from the dorsal raphe to ventral tegmental area dopamine neurons. Nat. Commun. 5, 5390 (2014).
Kessner, S. S. et al. Somatosensory deficits after ischemic stroke. Stroke 50, 1116–1123 (2019).
Carey, L. M., Matyas, T. A. & Oke, L. E. Sensory loss in stroke patients: effective training of tactile and proprioceptive discrimination. Arch. Phys. Med. Rehabil. 74, 602–611 (1993).
Wolny, T., Linek, P. & Michalski, P. Inter-rater reliability of two-point discrimination in acute stroke patients. NeuroRehabilitation 41, 127–134 (2017).
Qin, S., Meng, Q. & Yu, H. Advances in sensory feedback based on transcutaneous electrical stimulation. In 2024 17th International Convention on Rehabilitation Engineering and Assistive Technology (i-CREATe). https://doi.org/10.1109/i-CREATe62067.2024.10776188 (IEEE, 2024).
Schabrun, S. & Hillier, S. Evidence for the retraining of sensation after stroke: a systematic review. Clin. Rehabil. 23, 27–39 (2009).
Serrada, I., Hordacre, B. & Hillier, S. L. Does sensory retraining improve sensation and sensorimotor function following stroke: a systematic review and meta-analysis. Front. Neurosci. 13, 402 (2019).
Flor, H. et al. Phantom-limb pain as a perceptual correlate of cortical reorganization following arm amputation. Nature 375, 482–484 (1995).
Juottonen, K. et al. Altered central sensorimotor processing in patients with complex regional pain syndrome. Pain 98, 315–323 (2002).
Lotze, M., Flor, H., Grodd, W., Larbig, W. & Birbaumer, N. Phantom movements and pain. An fMRI study in upper limb amputees. Brain 124, 2268–2277 (2001).
Maihöfner, C., Handwerker, H. O., Neundörfer, B. & Birklein, F. Patterns of cortical reorganization in complex regional pain syndrome. Neurology 61, 1707–1715 (2003).
Duncan, R. O. & Boynton, G. M. Tactile hyperacuity thresholds correlate with finger maps in primary somatosensory cortex (S1). Cereb. Cortex 17, 2878–2891 (2007).
Srivastava, A. et al. Stroke with supernumerary phantom limb: case study, review of literature and pathogenesis. Acta Neuropsychiatr. 20, 256–264 (2008).
Rognini, G. et al. Multisensory bionic limb to achieve prosthesis embodiment and reduce distorted phantom limb perceptions. J. Neurol. Neurosurg. Psychiatry 90, 833–836 (2019).
Maura, R. M. et al. Literature review of stroke assessment for upper-extremity physical function via EEG, EMG, kinematic, and kinetic measurements and their reliability. J. Neuroeng. Rehabil. 20, 21 (2023).
Borzelli, D., Boarini, V. & Casile, A. A quantitative assessment of the hand kinematic features estimated by the oculus Quest 2. Sci. Rep. 15, 8842 (2025).
Serino, A. et al. Body part-centered and full body-centered peripersonal space representations. Sci. Rep. 5, 18603 (2015).
D’Anna, E. et al. A somatotopic bidirectional hand prosthesis with transcutaneous electrical nerve stimulation based sensory feedback. Sci. Rep. 7, 10930 (2017).
Chai, G., Sui, X., Li, S., He, L. & Lan, N. Characterization of evoked tactile sensation in forearm amputees with transcutaneous electrical nerve stimulation. J. Neural Eng. 12, 066002 (2015).
Chai, G., Zhang, D. & Zhu, X. Developing non-somatotopic phantom finger sensation to comparable levels of somatotopic sensation through user training with electrotactile stimulation. IEEE Trans. Neural Syst. Rehabil. Eng. 25, 469–480 (2017).
Basla, C., Chee, L., Valle, G. & Raspopovic, S. A non-invasive wearable sensory leg neuroprosthesis: mechanical, electrical and functional validation. J. Neural Eng. 19, 016008 (2022).
Chee, L. et al. Optimally-calibrated non-invasive feedback improves amputees’ metabolic consumption, balance and walking confidence. J. Neural Eng. 19, 046049 (2022).
Petrini, F. M. et al. Enhancing functional abilities and cognitive integration of the lower limb prosthesis. Sci. Transl. Med. 11, eaav8939 (2019).
Lyle, R. C. A performance test for assessment of upper limb function in physical rehabilitation treatment and research. Int. J. Rehabil. Res. 4, 483–492 (1981).
Mahoney, F. I. & Barthel, D. W. Functional evaluation: the Barthel Index. Md State Med. J. 14, 61–65 (1965).
Rizzolatti, G., Fadiga, L., Fogassi, L. & Gallese, V. The space around us. Science 277, 190–191 (1997).
Cashin, A. G. & McAuley, J. H. Measuring two-point discrimination threshold with a caliper. J. Physiother. 63, 186 (2017).
Hsieh, Y.-W. et al. Establishing the minimal clinically important difference of the Barthel Index in stroke patients. Neurorehabil. Neural Repair 21, 233−238 (2007).
Aurucci, G. V. et al. Immersive virtual reality with synchronous neurostimulation for upper-limb recovery after stroke: a randomized feasibility trial. Zenodo. https://doi.org/10.5281/zenodo.16043228 (2025).
Acknowledgements
The authors are immensely grateful to the volunteers who freely donated their time to the advancement of knowledge and to a better future for stroke treatment and assessment. The authors are grateful to M. Relic for her help throughout the experimental sessions. All authors had complete access to data. All authors authorized submission of the manuscript, and the final submission decision was made by the corresponding author.
Funding
This project has received the following funding: Swiss National Science Foundation (SNSF) (MOVEIT no. 197271). Open access funding provided by Medical University of Vienna.
Author information
Authors and Affiliations
Contributions
G.V.A. designed the platform, performed all the experiments and all the analyses, made the figures and wrote the manuscript. O.D. recruited participants, performed all the experiments and wrote the manuscript. A.C. and N.S. contributed to experiments and analysis and wrote the manuscript. T.D.T. contributed to experiments. M.D.A.C. and H.Y. helped in the design of the platform. L.K. recruited participants, discussed the protocol and results and reviewed the manuscript. S.R. designed the study, supervised the experiments, supervised the analyses, discussed the results and wrote the manuscript. All authors authorized submission of the manuscript, and the final submission decision was made by the corresponding author.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Nature Medicine thanks Emilia Ambrosini, Marco Iosa, David Reinkensmeyer and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Primary Handling Editor: Jerome Staal, in collaboration with the Nature Medicine team.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data
Extended Data Fig. 1 Randomized feasibility study protocol.
Participants were randomized into two groups: MultiSensy and Conventional Rehabilitation. Both groups underwent 12 rehabilitation sessions over three weeks, matched in dose and type of movements performed. In the MultiSensy group, each session began with an electrical stimulation calibration, followed by 6–8 personalized rehabilitation games, each lasting 4 min. Assessments were conducted at T0 (Day 1, baseline, pre-intervention), T1 (Day 10, after six sessions), T2 (Day 19, post-intervention), and T3 (Day 33, follow-up, two weeks post-intervention). The assessment battery included motor-functional tests (FMUE, ARAT, Barthel Index), sensory evaluation (2PD), and body representation tests (Body Landmark and Peri-Personal Space).
Extended Data Fig. 2 Body Landmark validation.
A) BL validation setup and distances of interest. Baseline validation setup and distances of interest. During VR immersion, healthy controls placed their hand on a table. The real-world positions of five landmarks were recorded using a millimeter grid beneath the arm, while VR landmark positions were measured within the virtual environment. Arm and hand dimensions were assessed in both real (pink) and VR-based (blue) conditions. B) BL indexes systematics errors. Meta Quest 2and HTC Vive Pro errors in computing the indexes of interest are reported. The difference between VR-based and real indexes is shown for N = 9 healthy controls (Meta Quest 2) and N = 7 (HTC Vive Pro). Mean and SEM are presented. C) BL results from the proof-of-concept study - validation. For each index, the Meta Quest 2 system error is reported alongside the improvement from T0 to T2 and T3 for N = 13 patients. Mean and SEM are shown. Two-sided independent t-tests were used to assess whether the observed improvements were significantly greater than the system error. D) BL results from pilot phase - validation. For each index, the HTC system error is reported alongside the improvement from the baseline and control condition to the VRstim condition N = 9 patients. Mean and SEM are shown. Two-sided independent t-tests were used to assess whether the observed improvements were significantly greater than the system error.
Supplementary information
Supplementary Information (download PDF )
Supplementary Results, Figs. 1–3, Tables 1–12 and study protocol.
Supplementary Video 1 (download MP4 )
Patient P03.
Supplementary Video 2 (download MP4 )
Patient P07.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/
About this article
Cite this article
Aurucci, G.V., Djordjevic, O., Cimolato, A. et al. Immersive virtual reality with synchronous neurostimulation for upper-limb recovery after stroke: a randomized feasibility trial. Nat Med (2026). https://doi.org/10.1038/s41591-026-04486-4
Received:
Accepted:
Published:
Version of record:
DOI: https://doi.org/10.1038/s41591-026-04486-4